Invasive Mucinous Carcinoma
Contents
Introduction
|
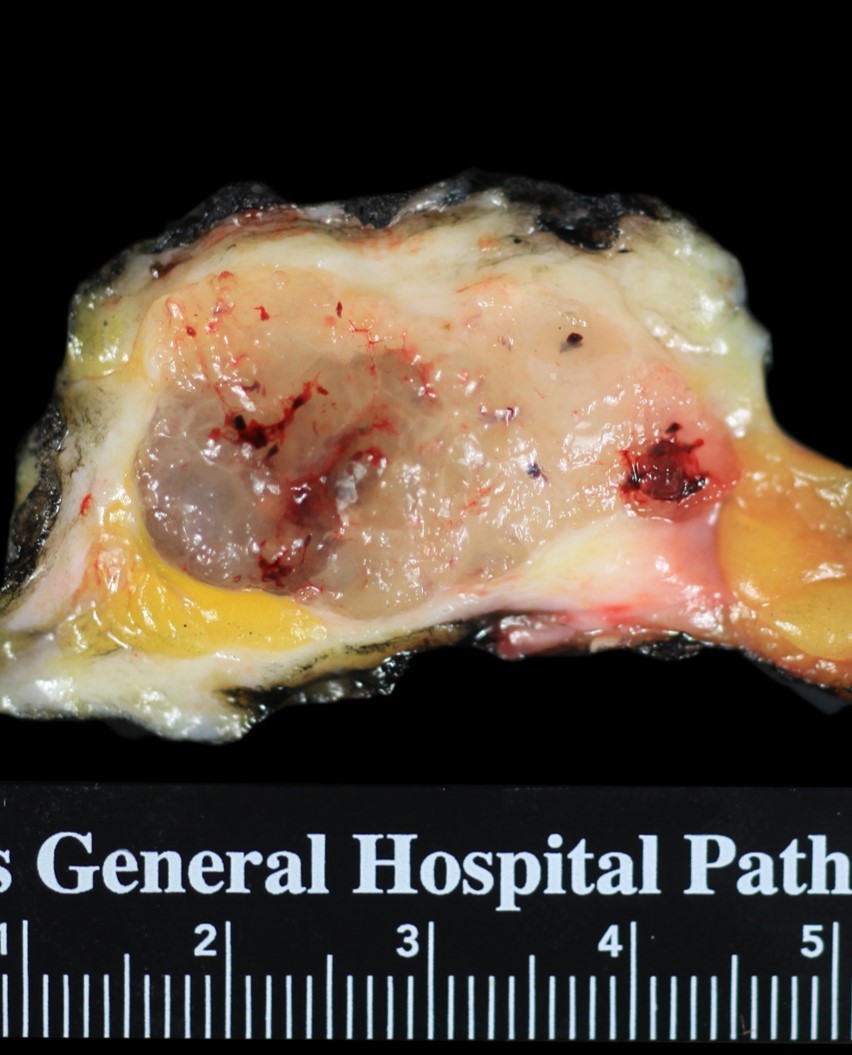
Definition: Mucinous carcinoma is a form of invasive ductal carcinoma in which the malignant cells secrete abundant mucin, which collects in large stromal pools. Only those carcinomas in which the mucin-producing component constitutes at least 90% of the mass qualify for the diagnosis of invasive mucinous carcinoma. Clinical Significance: Mucinous carcinoma produces a mass detectable by radiological imaging or physical examination. Patients with this form of carcinoma have a better prognosis than those with invasive ductal carcinoma of no special type. Gross Findings: Mucinous carcinoma forms a mostly well defined, irregular, soft, gelatinous mass of glistening, grey tissue. Microscopic Findings: Clusters of carcinoma cells sit within stromal collections of mucin. The typical invasive mucinous carcinoma stains for estrogen receptors. Differential Diagnosis: Invasive ductal carcinoma with mucin production (less than 90% of the carcinoma is mucin-producing), mucocoele-like lesion (no epithelial cells in the extravasated mucin) Discussion: This form of invasive ductal carcinoma features malignant ductal cells sitting in stromal mucin pools. Based on the cellularity of the carcinoma, one can recognize two types: conventional mucinous carcinoma, and cellular mucinous carcinoma. |
 |
Conventional Mucinious Carcinoma
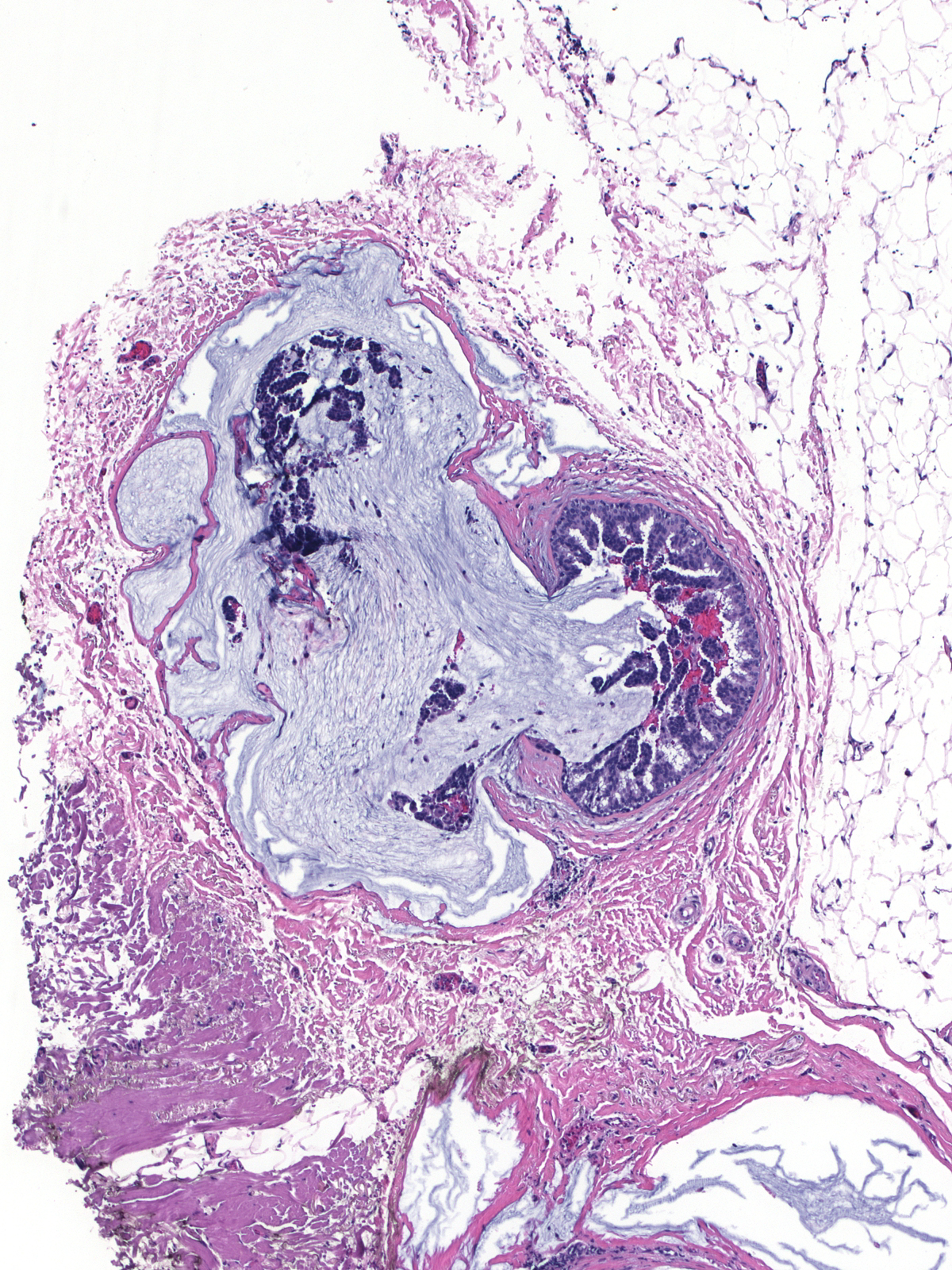
| Conventional mucinous carcinomas consist of only a few small clusters of cells widely dispersed in mucin. The mucin accounts for the majority of the size of the mass. | 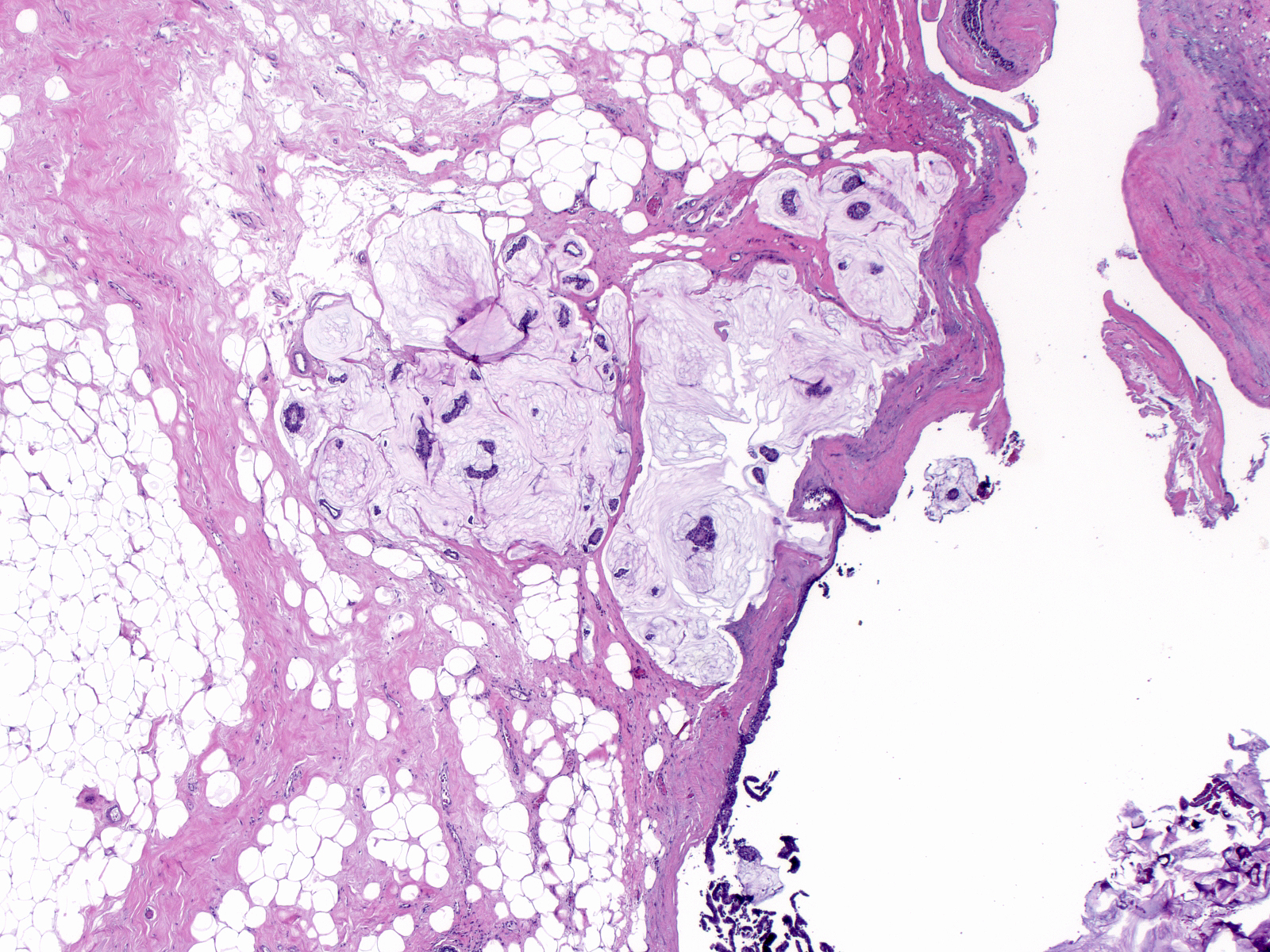 |
| The carcinoma cells form small, solid aggregates, oddly-shaped structures, and rings. | 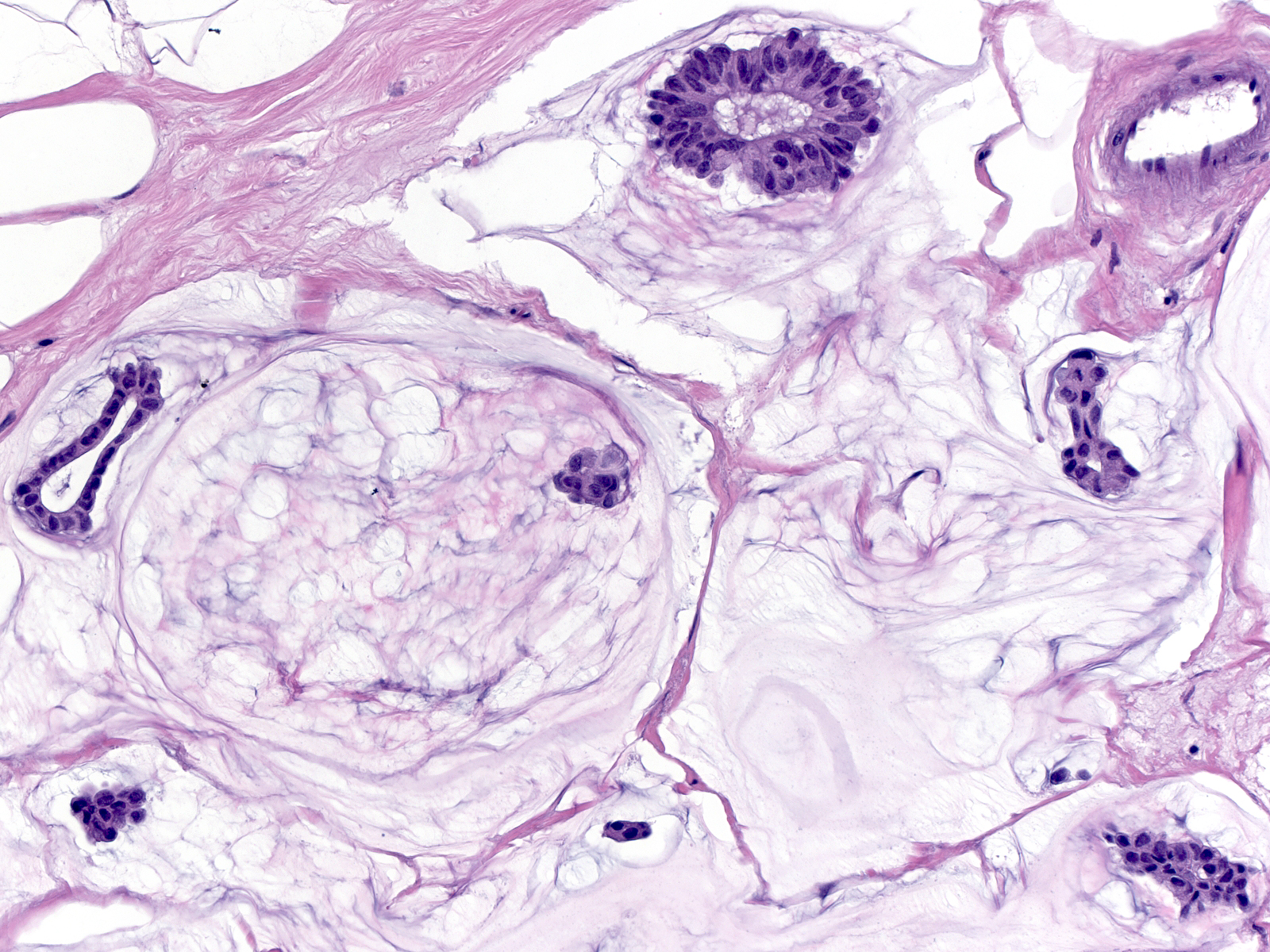 |
| In most examples, the cells exhibit low-grade cytological features. They appear slightly larger than normal cells and they possess slightly enlarged nuclei, homogeneous dark chromatin, inconspicuous nucleoli, and scant eosinophilic cytoplasm. The cytoplasm sometimes contains miniscule droplets of mucin, which imparts a foamy quality to it. | 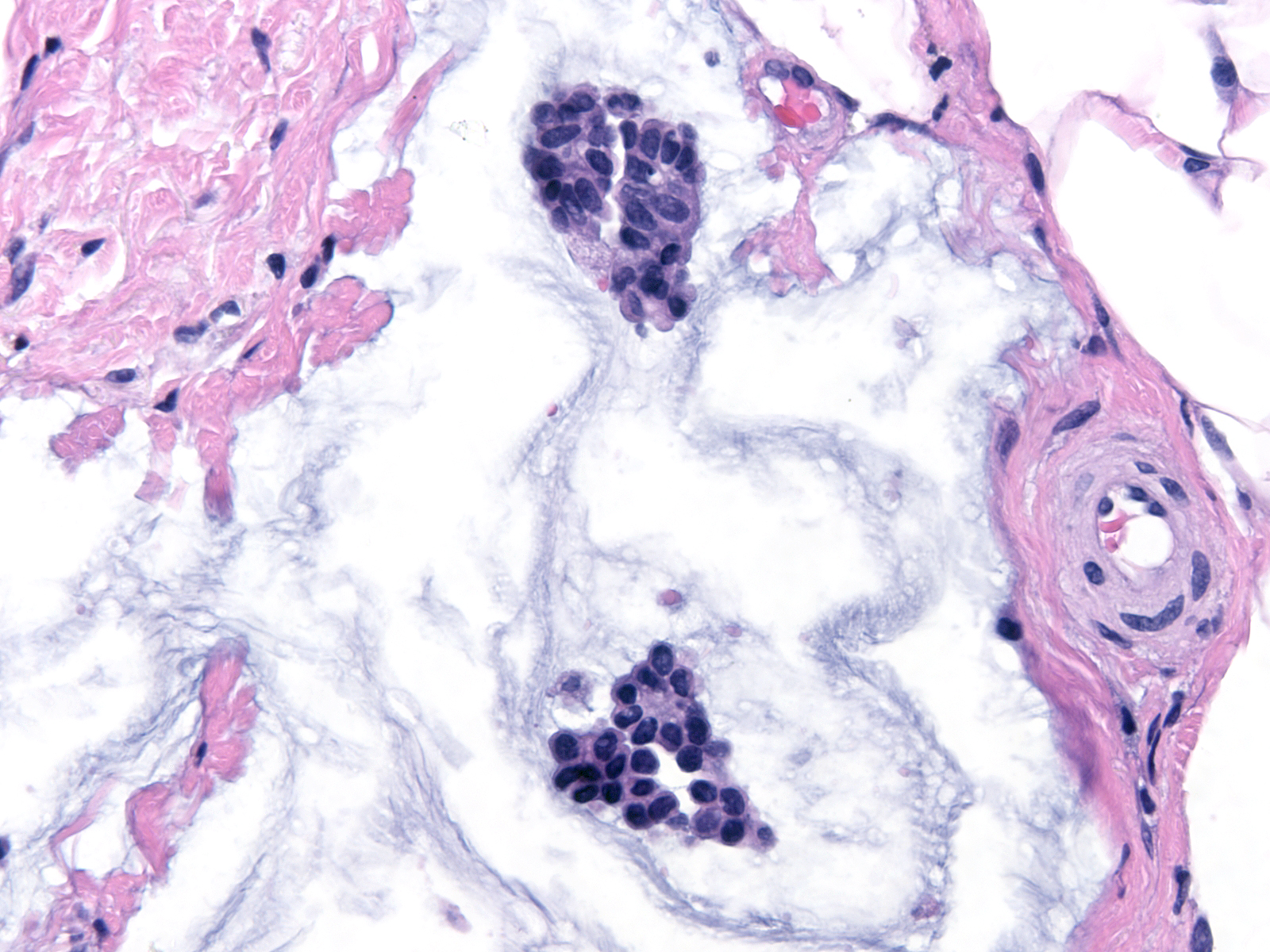 |
| Occasional cases demonstrate intermediate- or high-grade cytological atypia. | 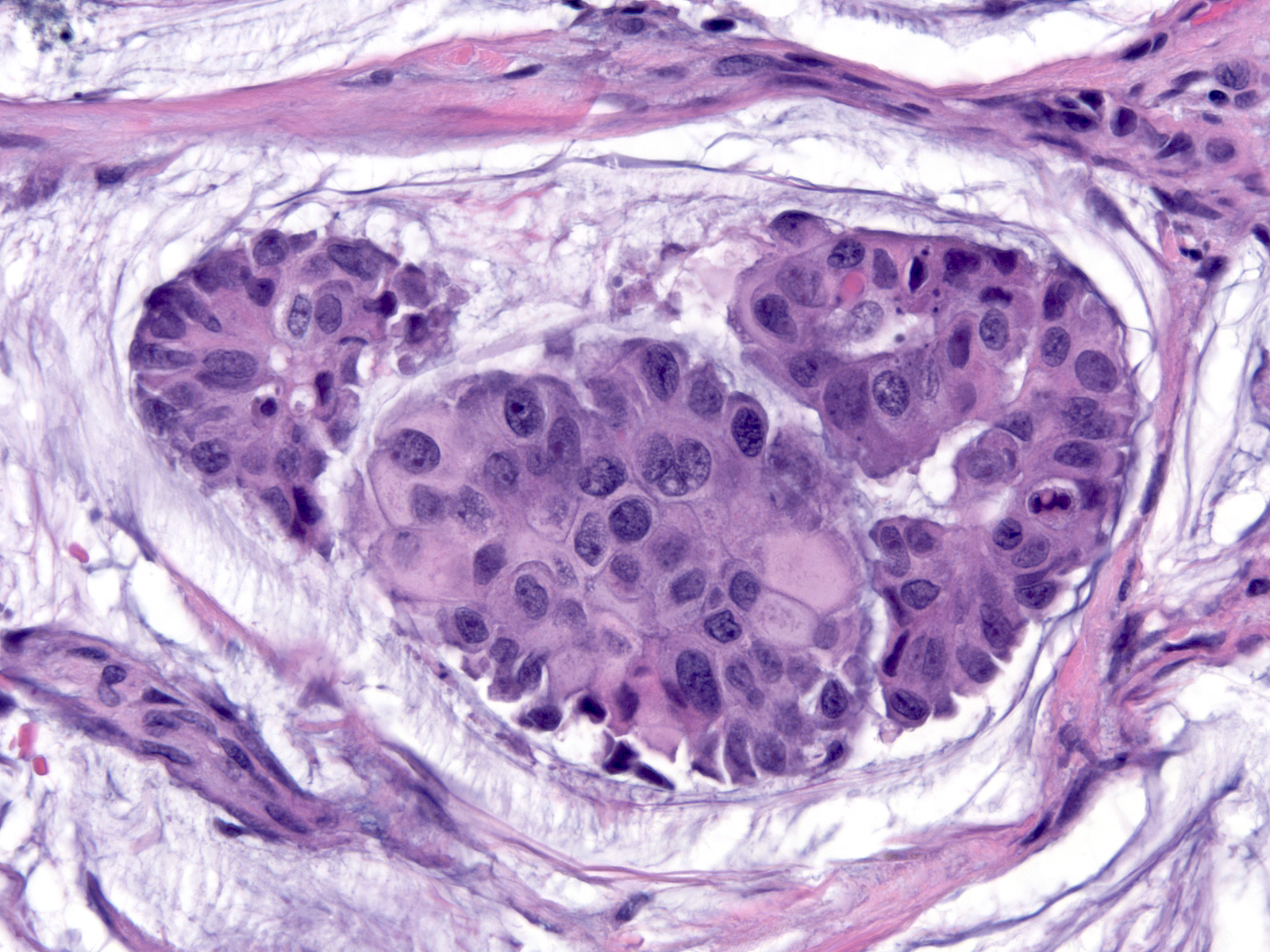 |
The collections of mucin often contain calcifications, strands of collagen, and small blood vessels.
 |
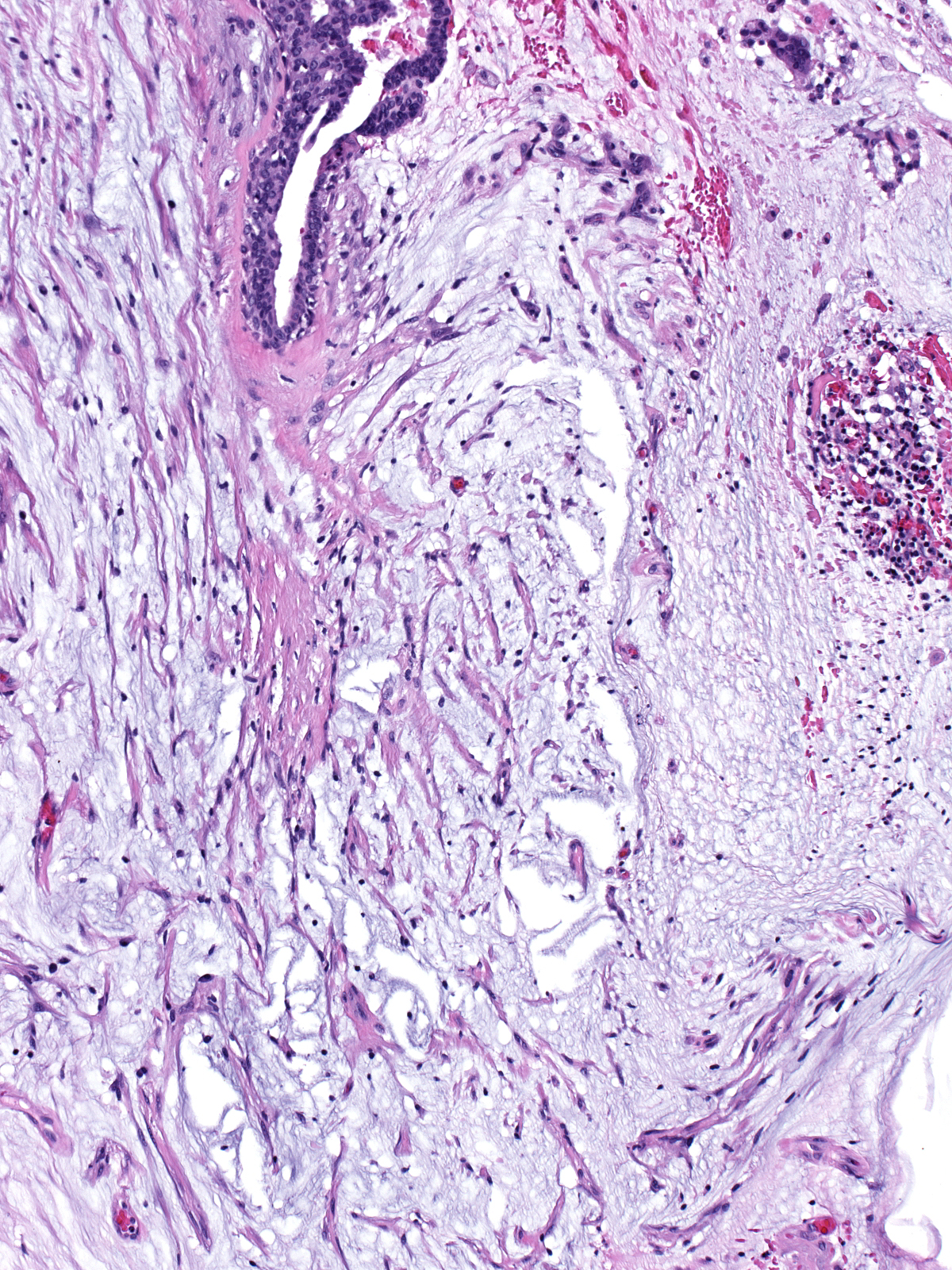 |
| The stroma surrounding the mucin may show chronic inflammation, foreign body giant cell reaction, and evidence of hemorrhage. | 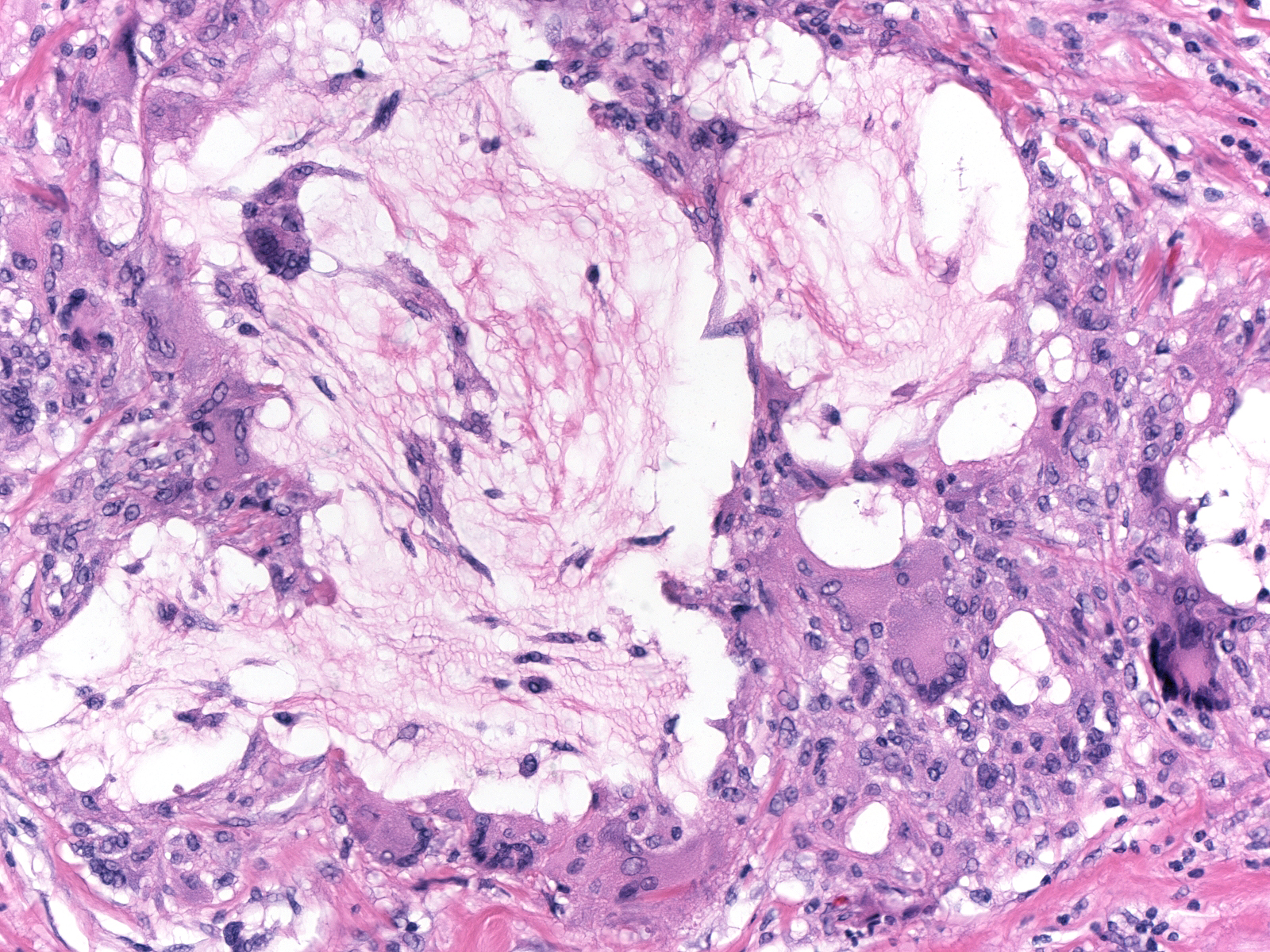 |
Iatrogenic interventions such as needle aspirations or core biopsies can disrupt the integrity of ducts and displace their contents into the stroma, and so can rough handling during excision. Displaced mucin can contain calcifications, strips of epithelial cells (sometimes with myoepithelial cells), epithelial clusters, and blood. One can sometimes recognize displaced duct contents when the displacement occurred during collection or handing of the specimen under examination; however, one has difficulty recognizing displaced material when the intervention took place a week or more prior to the current procedure. The presence of epithelial cells in linear strips or with attached myoepithelial cells within stromal mucin pools suggests that iatrogenic forces displaced these elements into the stroma. Stromal changes such as chronic inflammation and hemorrhage do not offer diagnostic information because both mucin displacement and genuine mucin extravasation evoke identical reactive stromal responses.
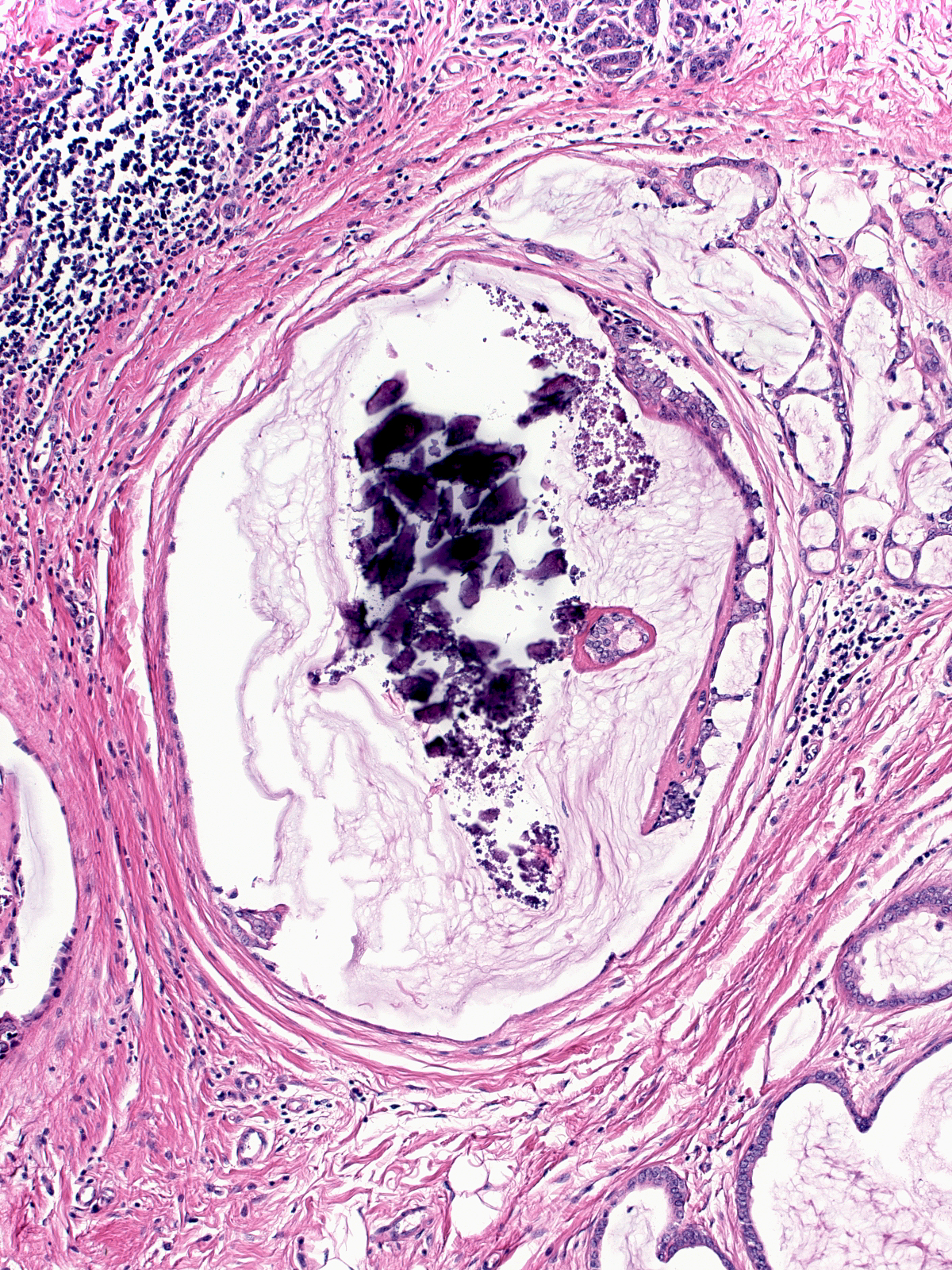
| The image to the right depicts a portion of a core biopsy specimen containing a mucocoele‑like lesion. The left gland appears intact; however, the biopsy has disrupted the wall of the right gland, and most of the mucin has spilled into the fat. As commonly happens, the epithelial lining adjacent to the point of rupture points towards the interior of the gland. | 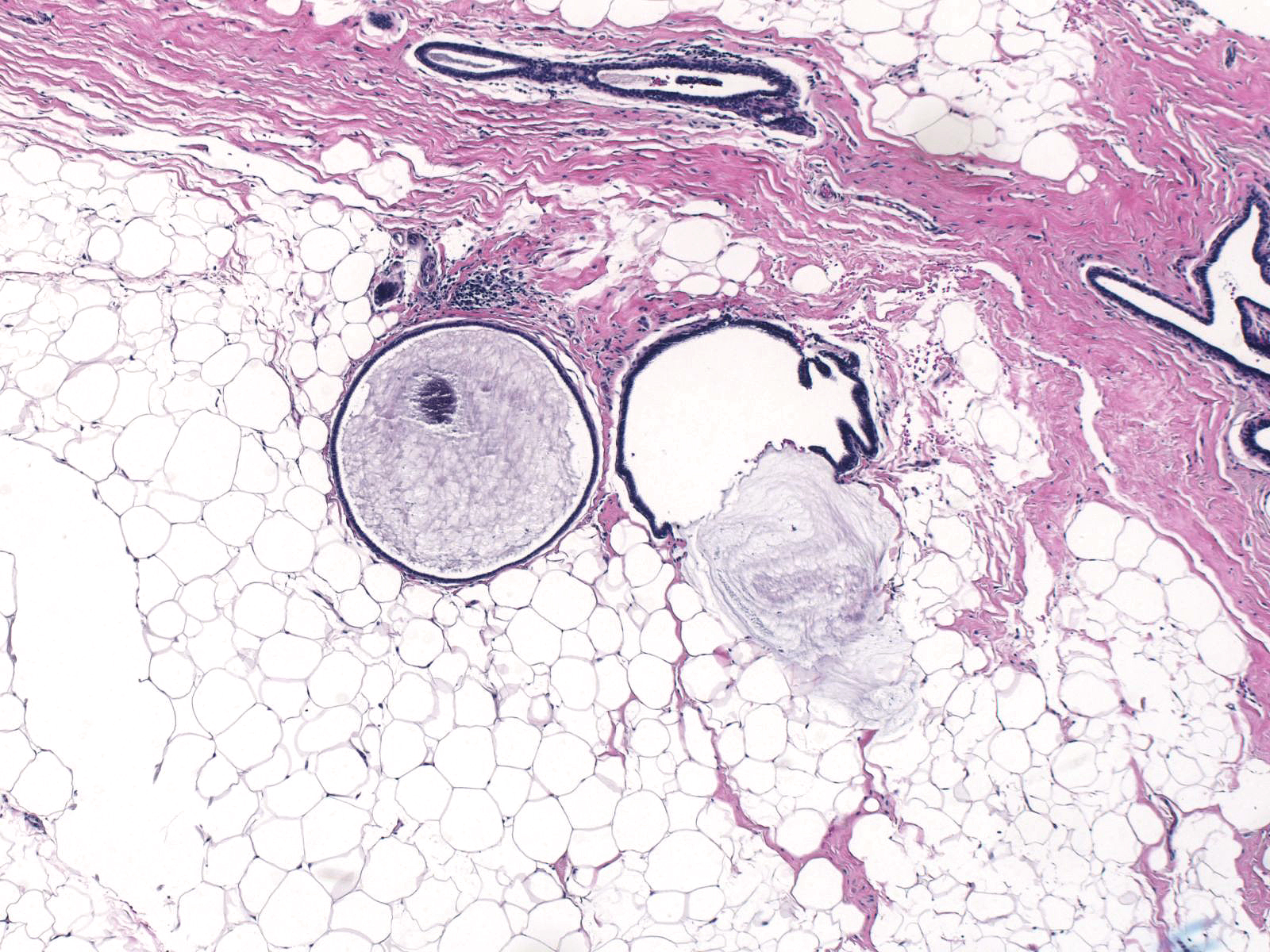 |
Cellular Mucinious Carcinoma
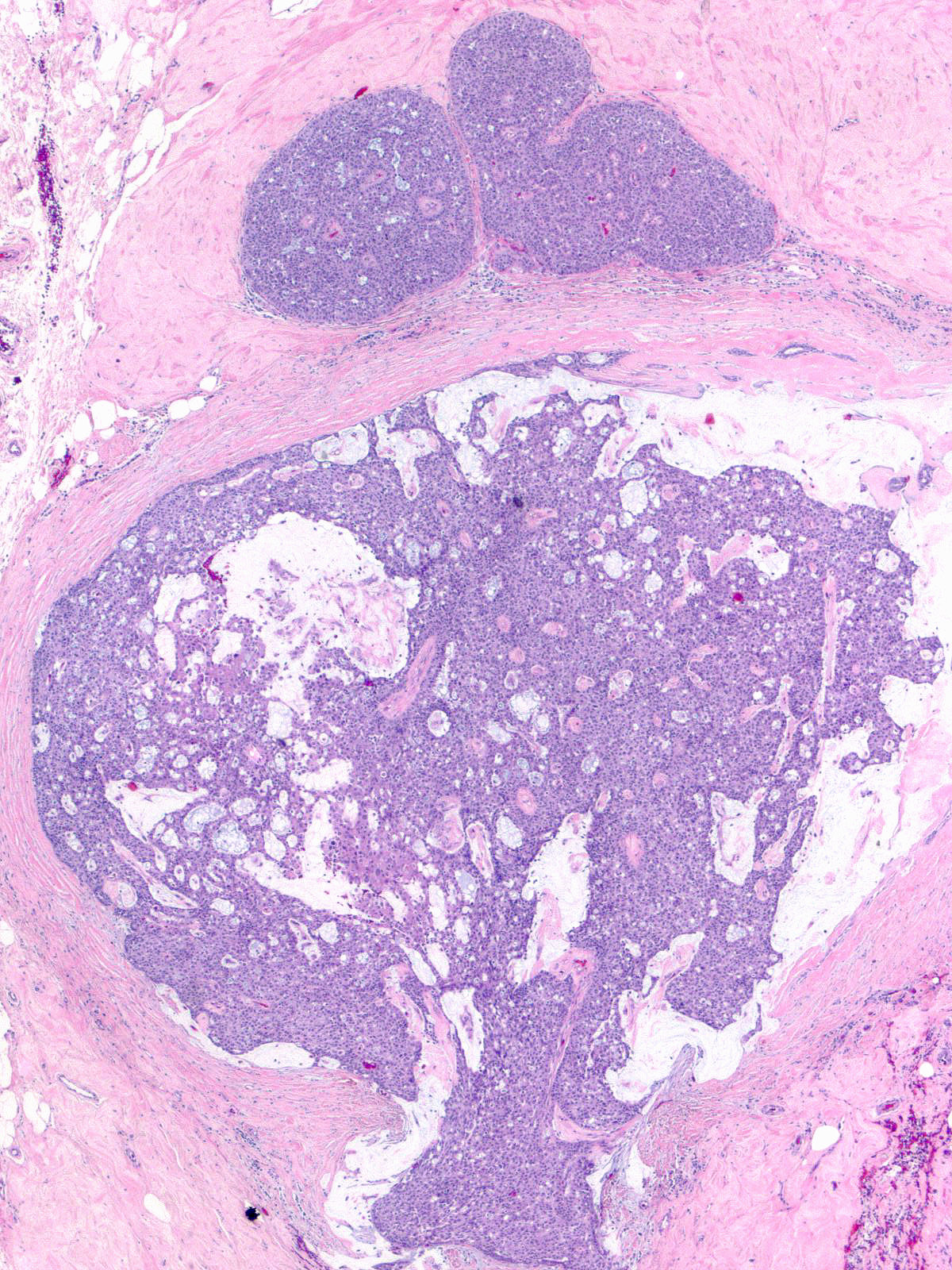
| Cellular mucinous carcinomas are similar to conventional mucinous carcinomas except that the former contain larger aggregates of carcinoma cells and lesser amounts of mucin than the latter. Cellular mucinous carcinomas usually occurs in postmenopausal women and usually displays endocrine characteristics. | 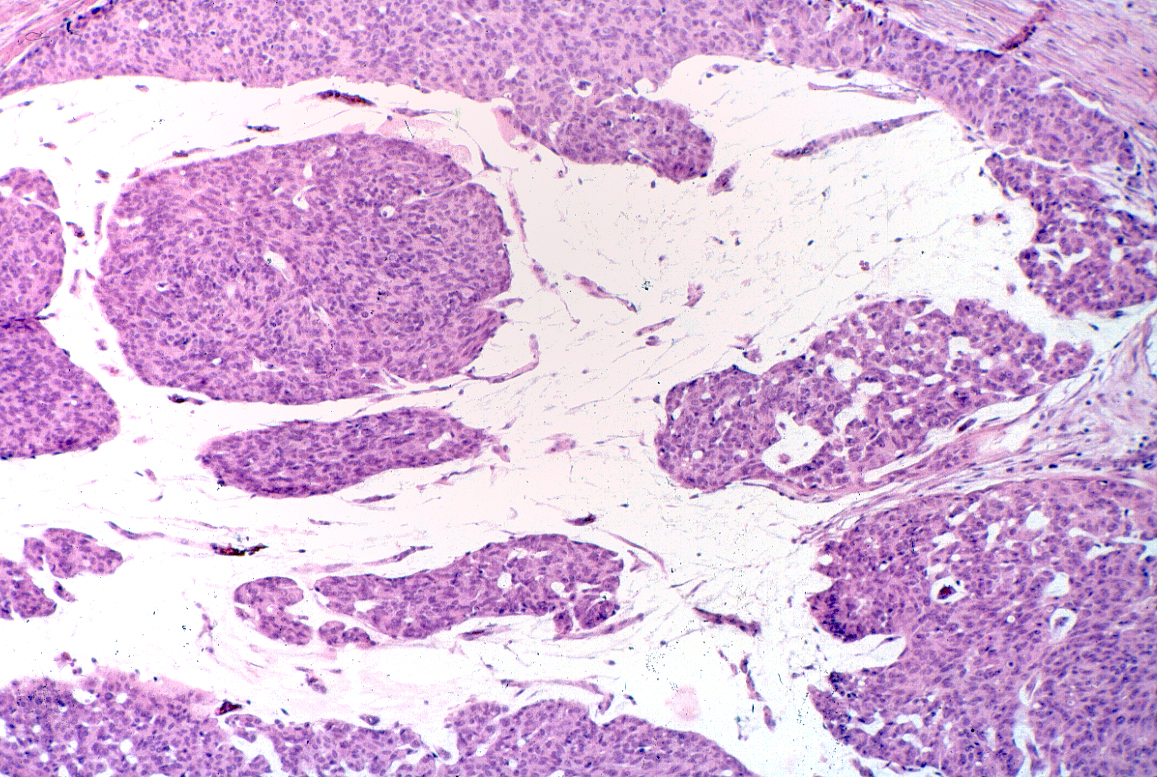 |
Origin
Both forms of invasive mucinous carcinoma arise from mucin-producing ductal carcinoma in-situ (DCIS).
 |
 |
Considerations Regarding Core Biopsy Specimens
Many breast carcinomas produce mucin. One should reserve the diagnosis of invasive mucinous carcinoma for carcinomas in which the mucin‑producing component accounts for 90% or more of the carcinomas. Core biopsies usually do not sample lesions thoroughly enough to determine the extent of a mucin‑producing component; consequently, one cannot make a confident diagnosis of invasive mucinous carcinoma based on a core biopsy sample.