General
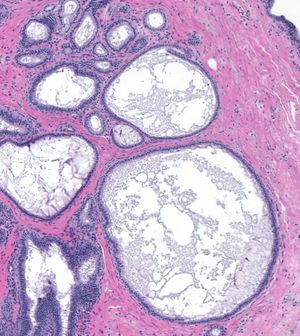
FEA expands the acini of a lobule.
- Definition: Flat epithelial atypia (FEA) represents the earliest recognizable morphological alteration in the formation of low-grade ductal carcinoma in-situ.
- Clinical Significance: FEA may produce calcifications, but often the lesion does not give rise to clinical signs or symptoms. When one diagnoses FEA in a core biopsy specimen, a surgeon ordinarily will carry out an excision of the biopsy site, and an oncologist may offer the patient antiestrogen therapy in an effort to forestall the development of breast carcinoma.
- Microscopic Findings: Four attributes characterize flat epithelial atypia.
- 1. The affected ductules and acini appear dilated and exhibit round shapes.
- 2. A single layer of ductal type cells lines the dilated glands.
- 3. The proliferative cells display low-grade cytological atypia.
- 4. The proportion of myoepithelial cells appears reduced.
- Differential Diagnosis: Blunt duct adenosis (no atypia, prominent myoepithelial cells), flat usual ductal hyperplasia (no atypia), apocrine cysts (no atypia, apocrine cytological features), fibrocystic changes with cysts (no atypia), atypical ductal hyperplasia (stratification) flat intermediate‑ or high‑grade carcinoma (marked atypia)
Origin of FEA
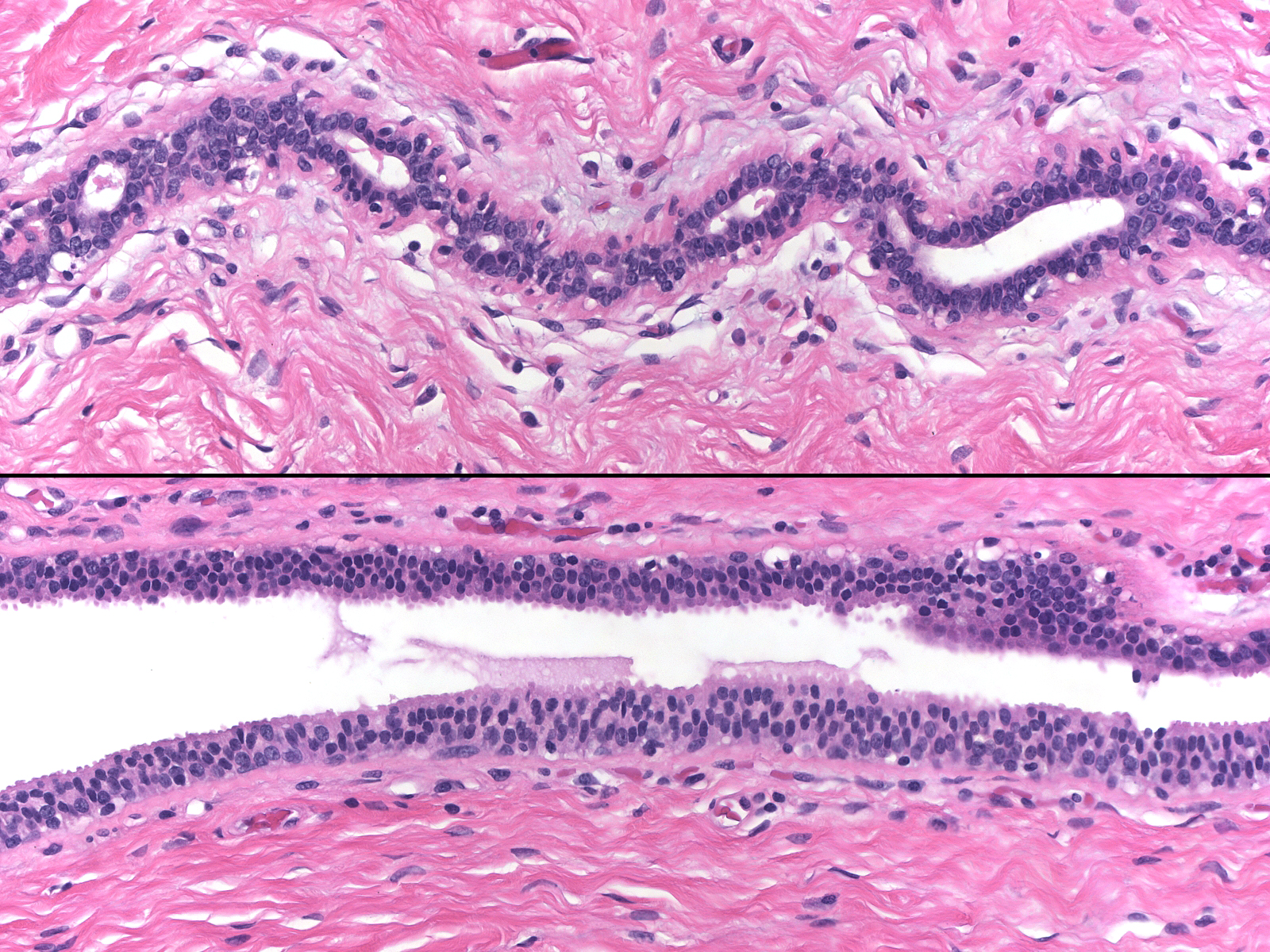
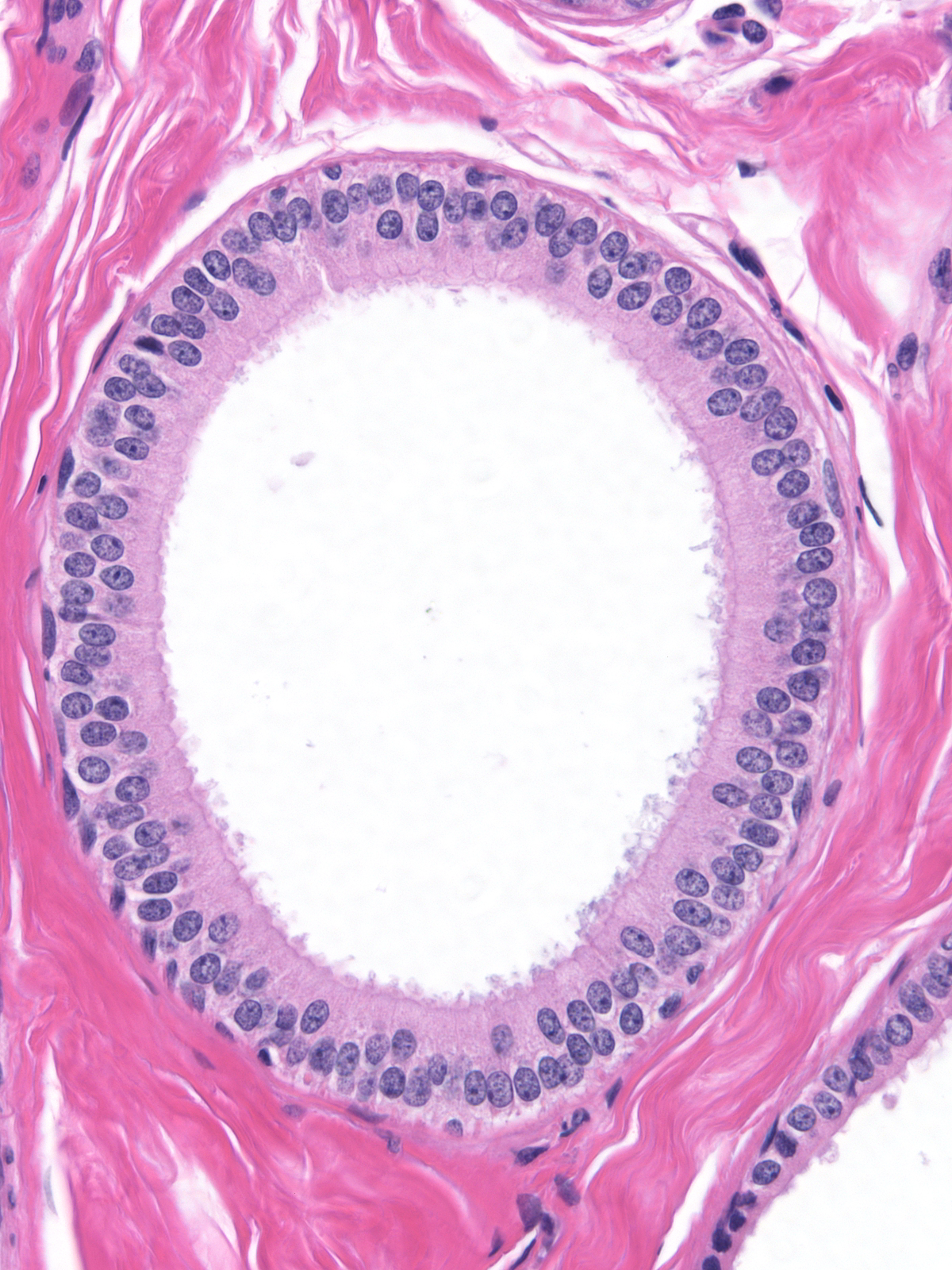
| The atypical ductal cells first become evident in the small ducts and ductules. |
 |
|
|
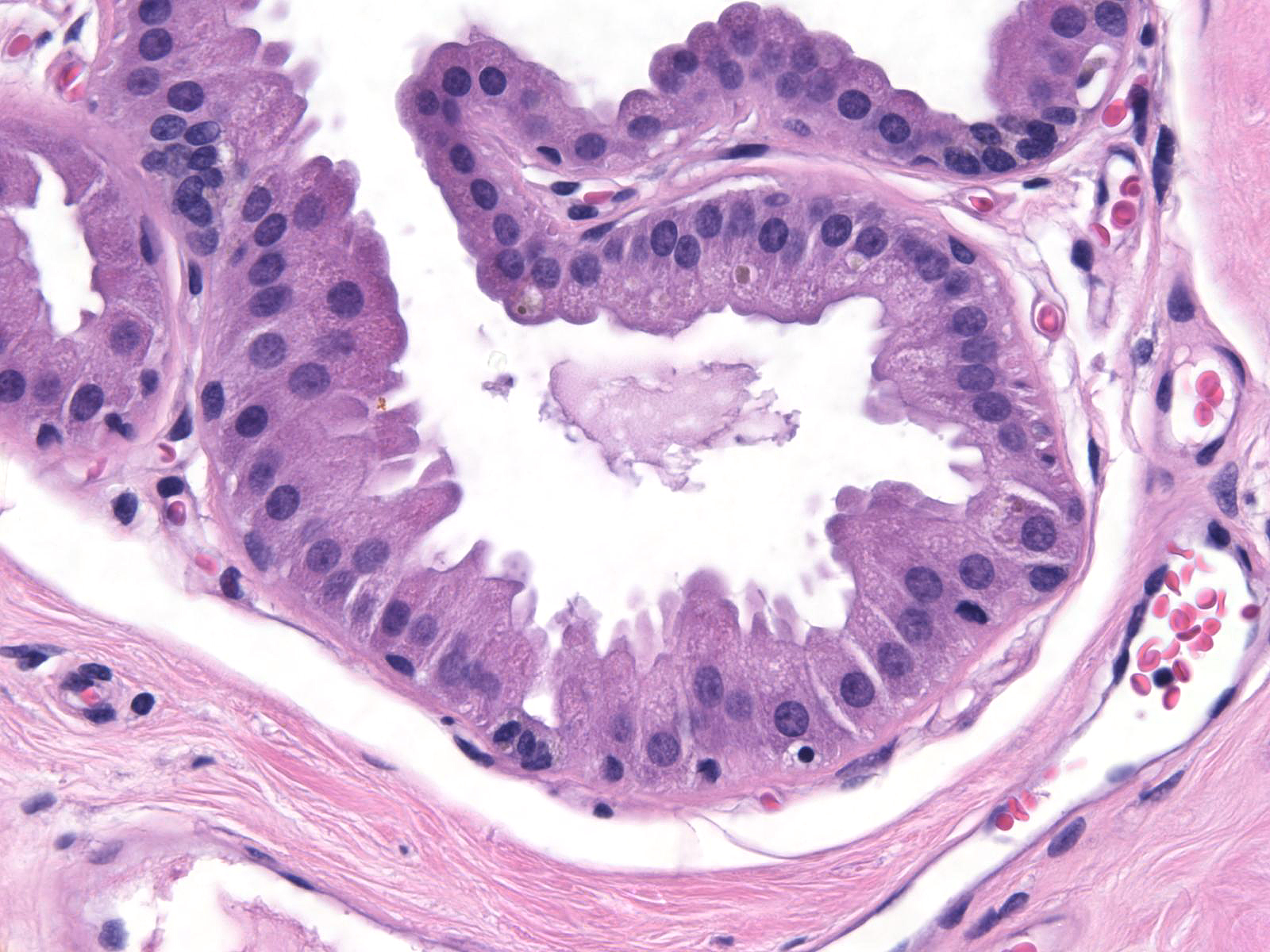
| Compare the uninvolved small duct (above) and the small duct involved by FEA (below). |
 |
|
|
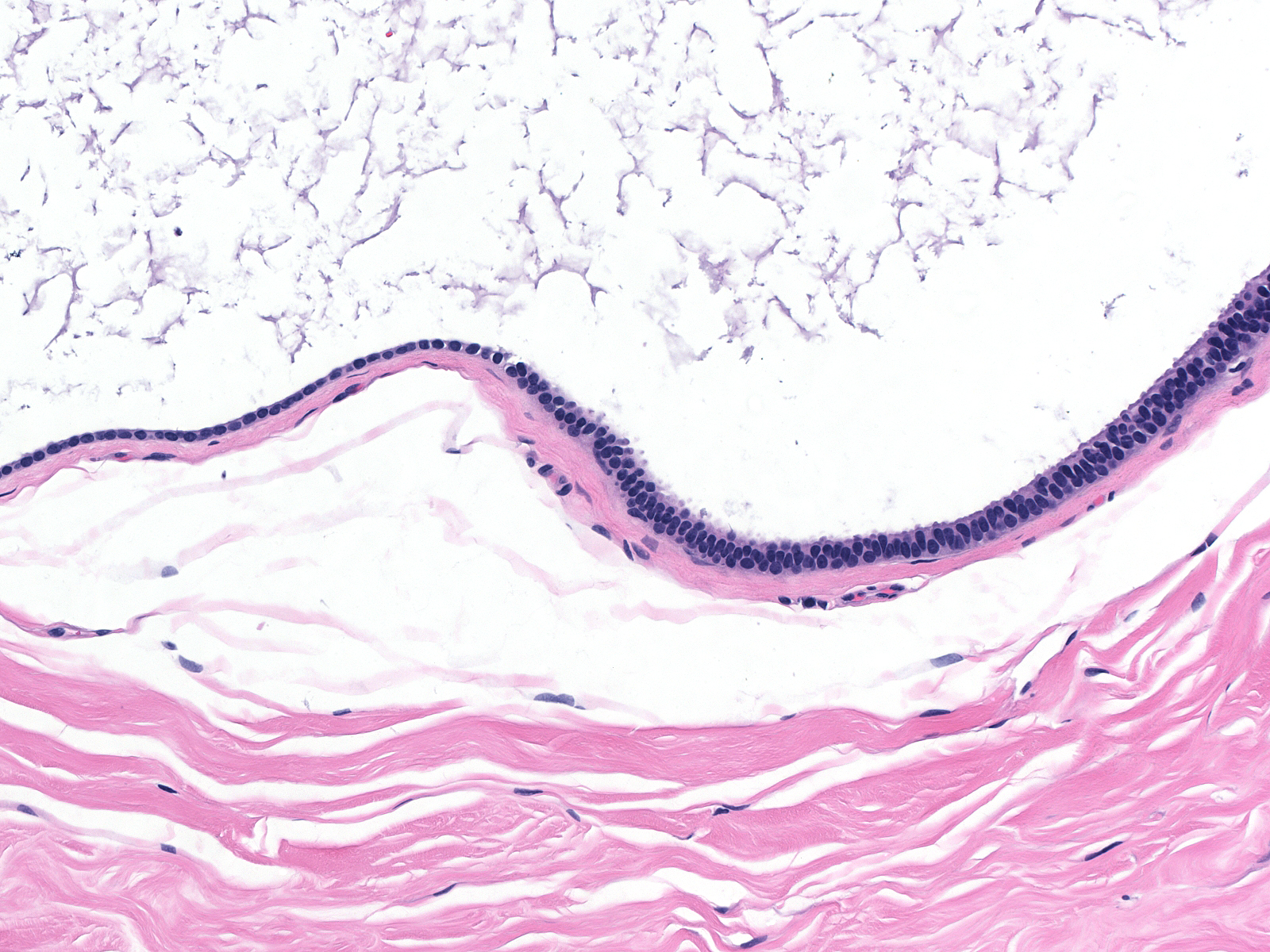
As the population expands into the lobule, atypia of the luminal acinar cells becomes evident.
 |
 |
| Early involvement of acini |
|
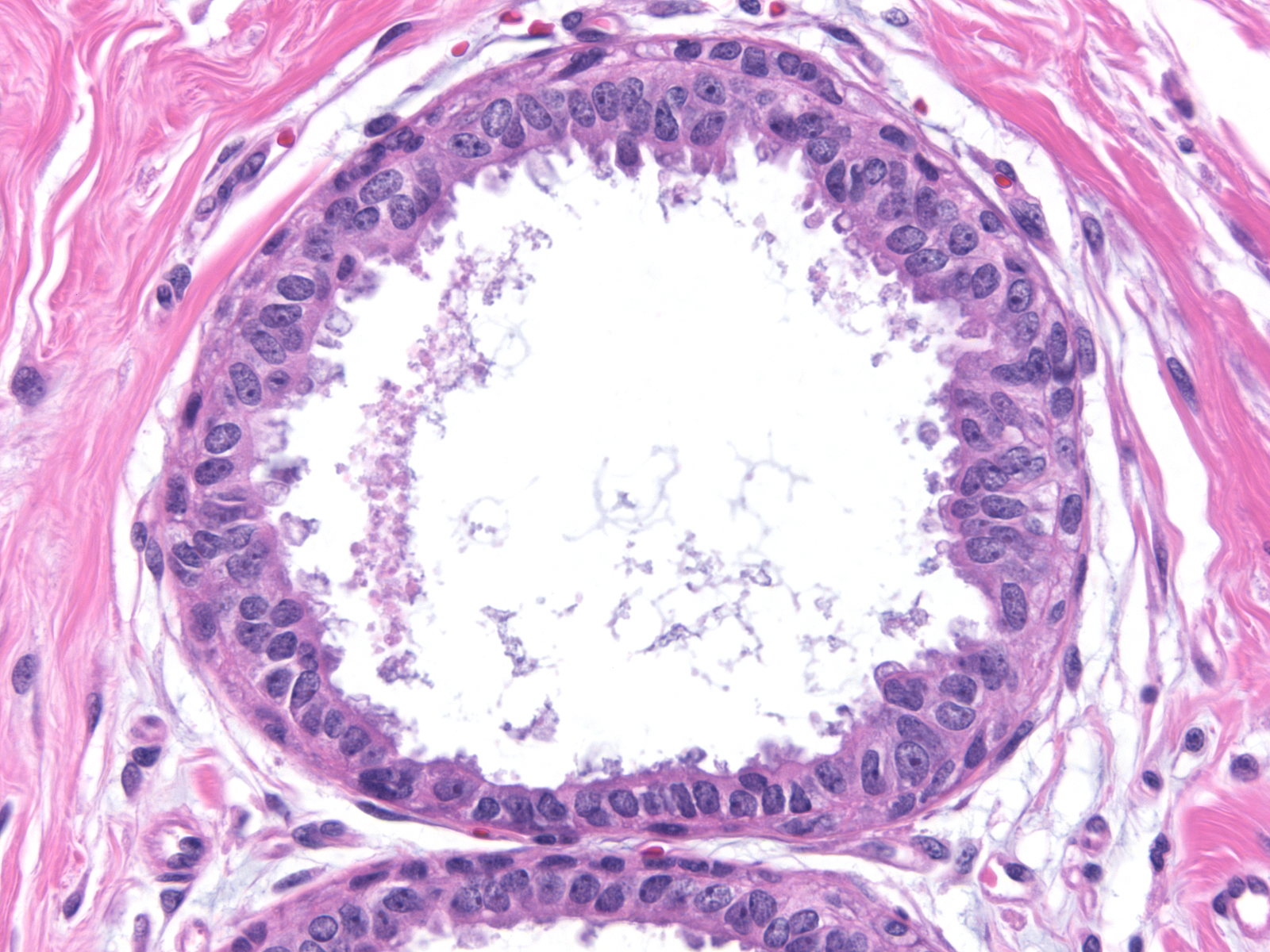
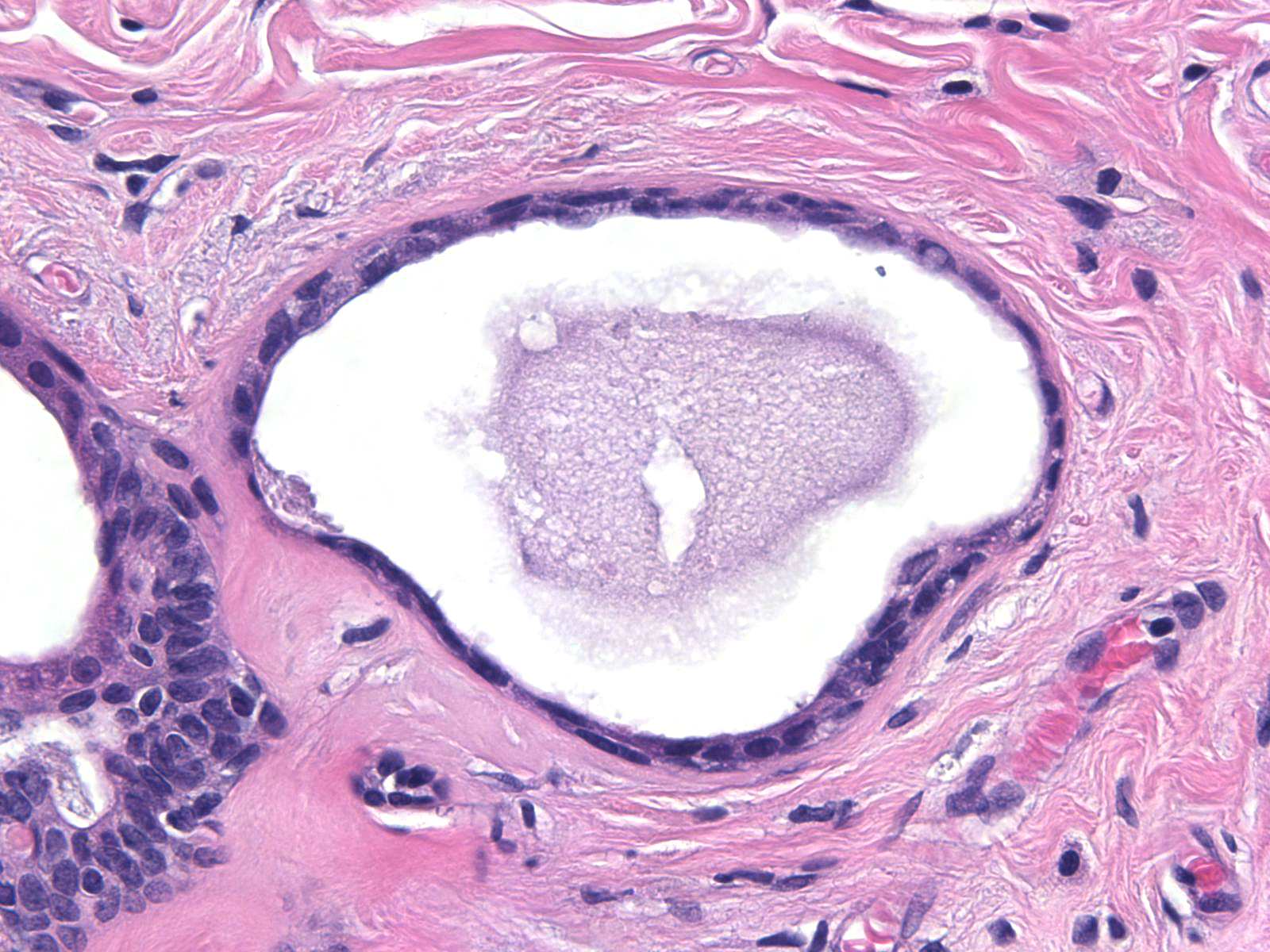
| Eventually, the affected glands enlarge and form a group of rounded structures. |
 |
|
|
| Calcifications often precipitate in the enlarged lumens. |
 |
|
|
Cytology and Architecture
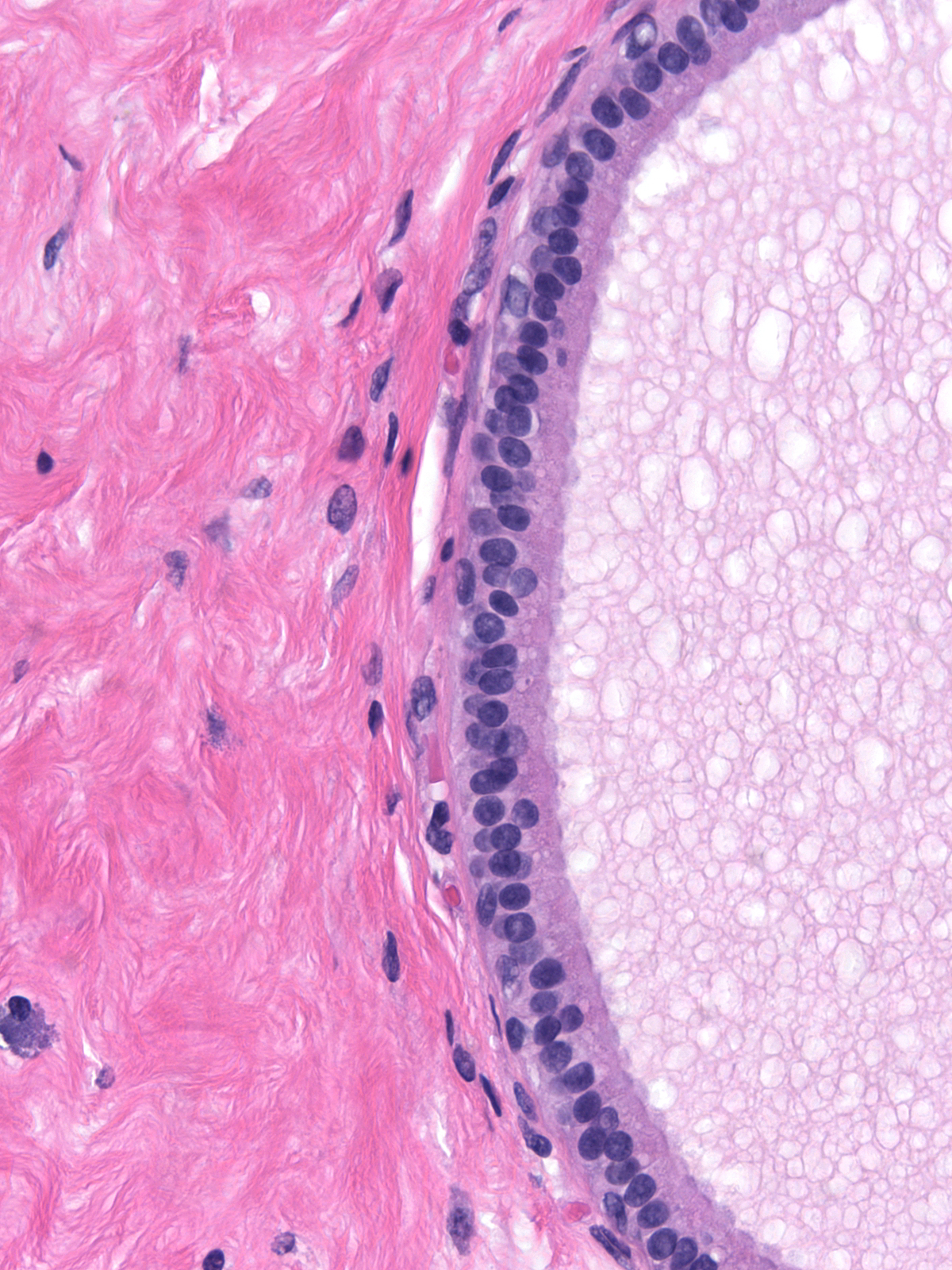
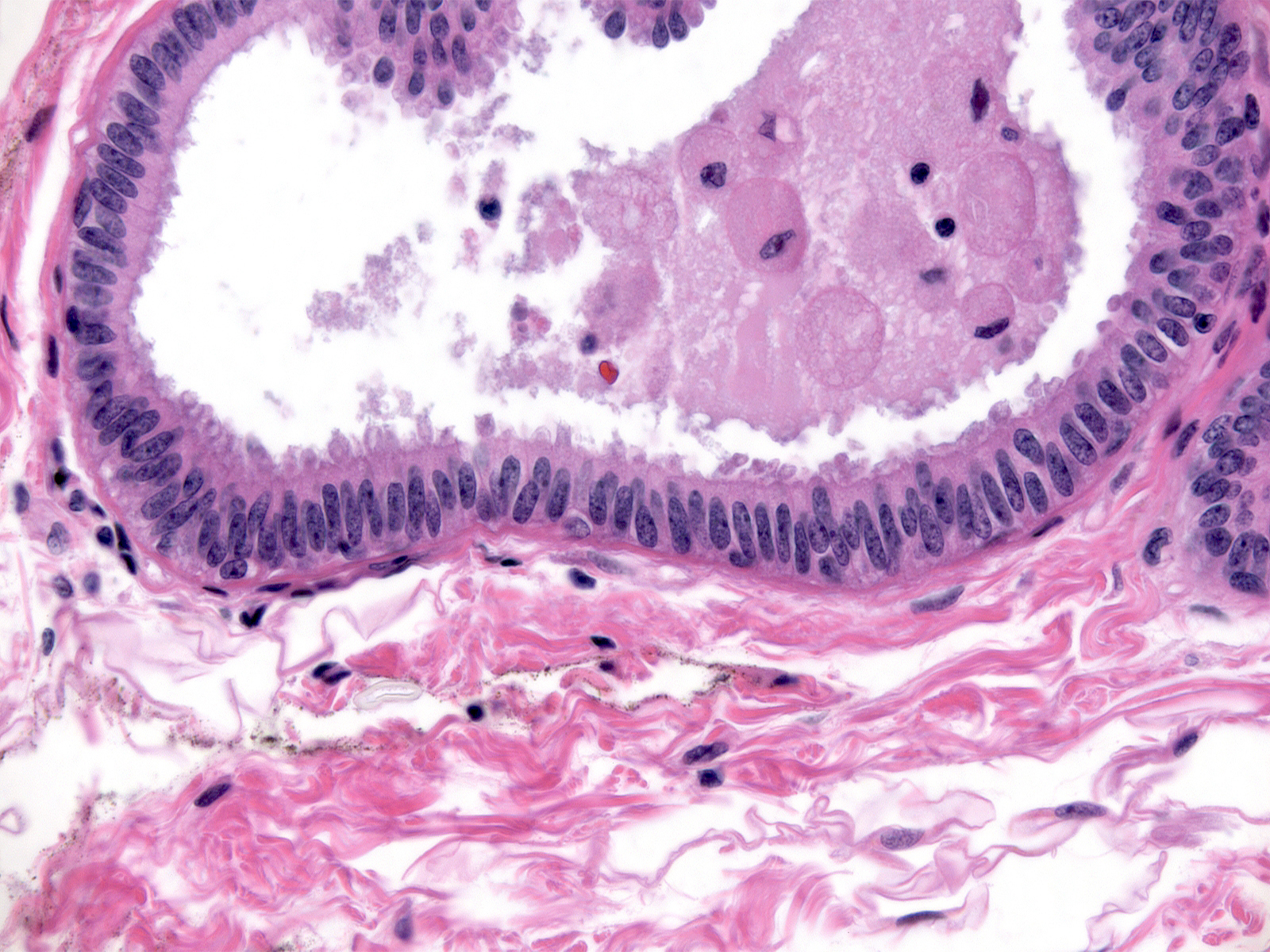
| The cells of FEA grow in a single layer. The nuclei tend to sit near the bases of the cells, and cytoplasm collects at the opposite poles so as to produce apical cytoplasmic compartments. |
 |
|
|
| The cells typically have a columnar shape and plenty of apical cytoplasm, but they can appear cuboidal or even flat and can possess only scant cytoplasm. |
 |
|
|
| Crowding of the cells can cause the nuclei to become oval or to sit at varying positions within the cells. Although such cells may appear stratified, they still form a single layer. |
 |
|
|
| The presence of genuine stratification and the formation of complex architectural structures exclude the diagnosis of flat atypia. One would make the diagnosis of atypical ductal hyperplasia in these circumstances. (Atypical ductal hyperplasia) |
 |
|
|
The neoplastic cells of FEA display low-grade atypia. The nuclei appear round or oval and smoothly contoured. They contain either finely dispersed dark chromatin or finely granular chromatin. The nucleoli appear inconspicuous.
 |
 |
| Finely dispersed dark chromatin |
Finely granular chromatin |
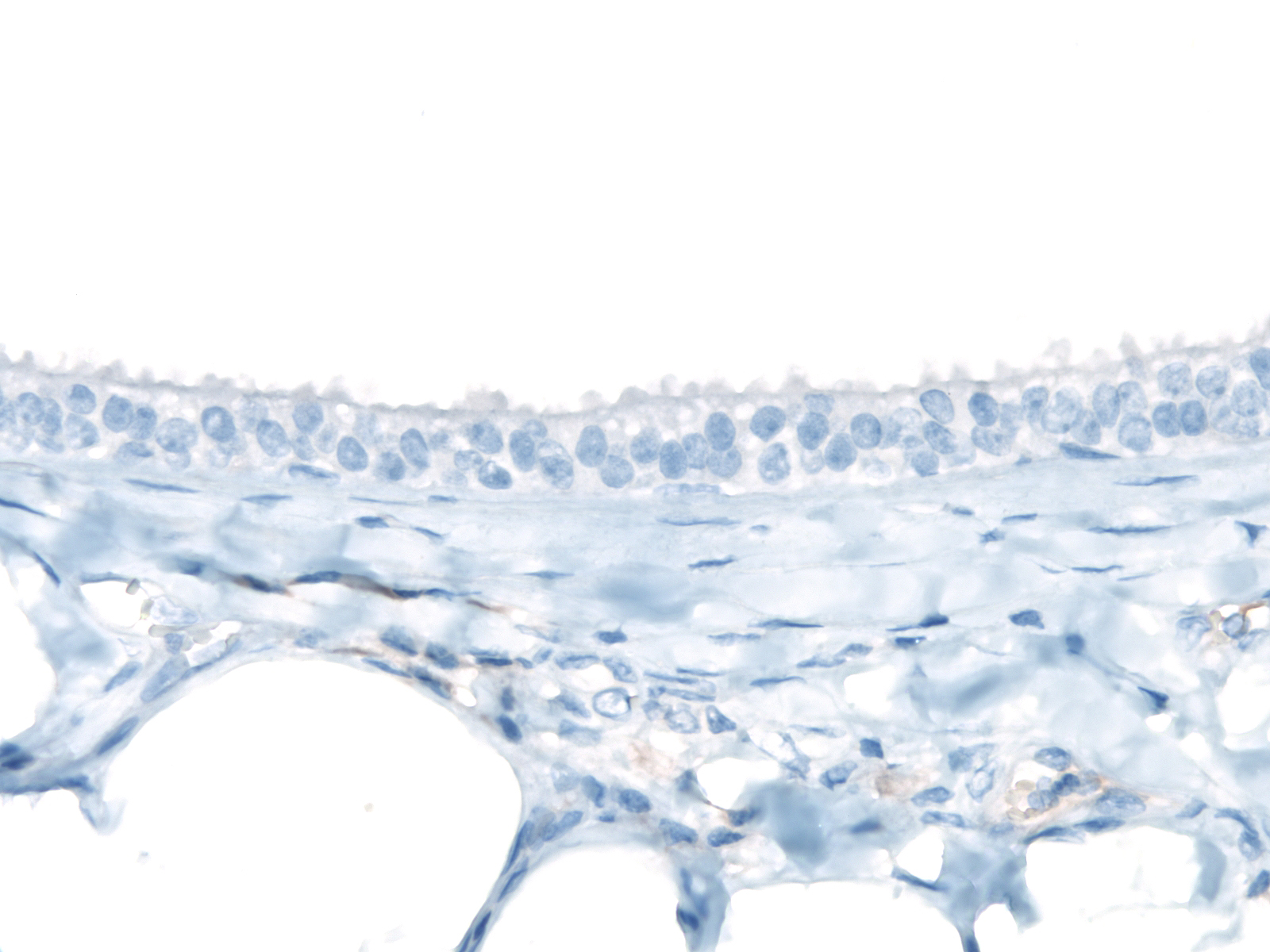
| The cells do not stain for CK 5/6. |
 |
|
|
| The presence of intermediate- or high-grade cytological atypia excludes the diagnosis of FEA. One would make the diagnosis of carcinoma in-situ in these situations. (High-grade ductal carcinoma in-situ (clinging carcinoma)) |
 |
|
|
| As the neoplastic luminal cells proliferate, the proportion of myoepithelial cells in the epithelium decreases. This feature varies somewhat, so the presence of residual, small myoepithelial cells, especially in small ducts, does not exclude the diagnosis of flat atypia if other findings support that interpretation. A layer of prominent myoepithelial cells, on the other hand, strongly argues against the diagnosis of FEA. |
 |
|
|
Differential Diagnosis
One must distinguish flat atypia from blunt duct adenosis, flat usual ductal hyperplasia, apocrine cysts, and cysts of fibrocystic changes. Blunt duct adenosis features prominent myoepithelial cells and luminal cells lacking cytological atypia (see the BDA page).
| Hyperplastic ductal cells growing in a flat pattern appear disheveled; they do not display the orderly arrangement that characterizes flat atypia. Hyperplastic nuclei vary in shape, they exhibit irregular contours, they sit at different positions in the cells, and their long axes do not display a consistent orientation with respect to the lumen. Moreover, hyperplastic cells do not possess atypical nuclei. (Flat usual ductal hyperplasia) |
 |
|
|
| The cells lining apocrine cysts contain copious amounts of granular, eosinophilic cytoplasm and characteristic nuclei. (Apocrine cyst) |
 |
|
|
| The cells lining cysts in fibrocystic changes appear flat; they contain only small amounts of cytoplasm; and they do not possess atypical nuclei. (Fibrocystic changes) |
 |
|
|
The differential diagnosis also includes atypical ductal hyperplasia and flat ductal carcinoma in‑situ. The usual examples of atypical ductal hyperplasia demonstrate architectural complexity not present in flat epithelial atypia. Flat intermediate- or high‑grade ductal carcinoma in‑situ displays a greater degree of cytological atypia than that exhibited by flat epithelial atypia
Rosen Triad
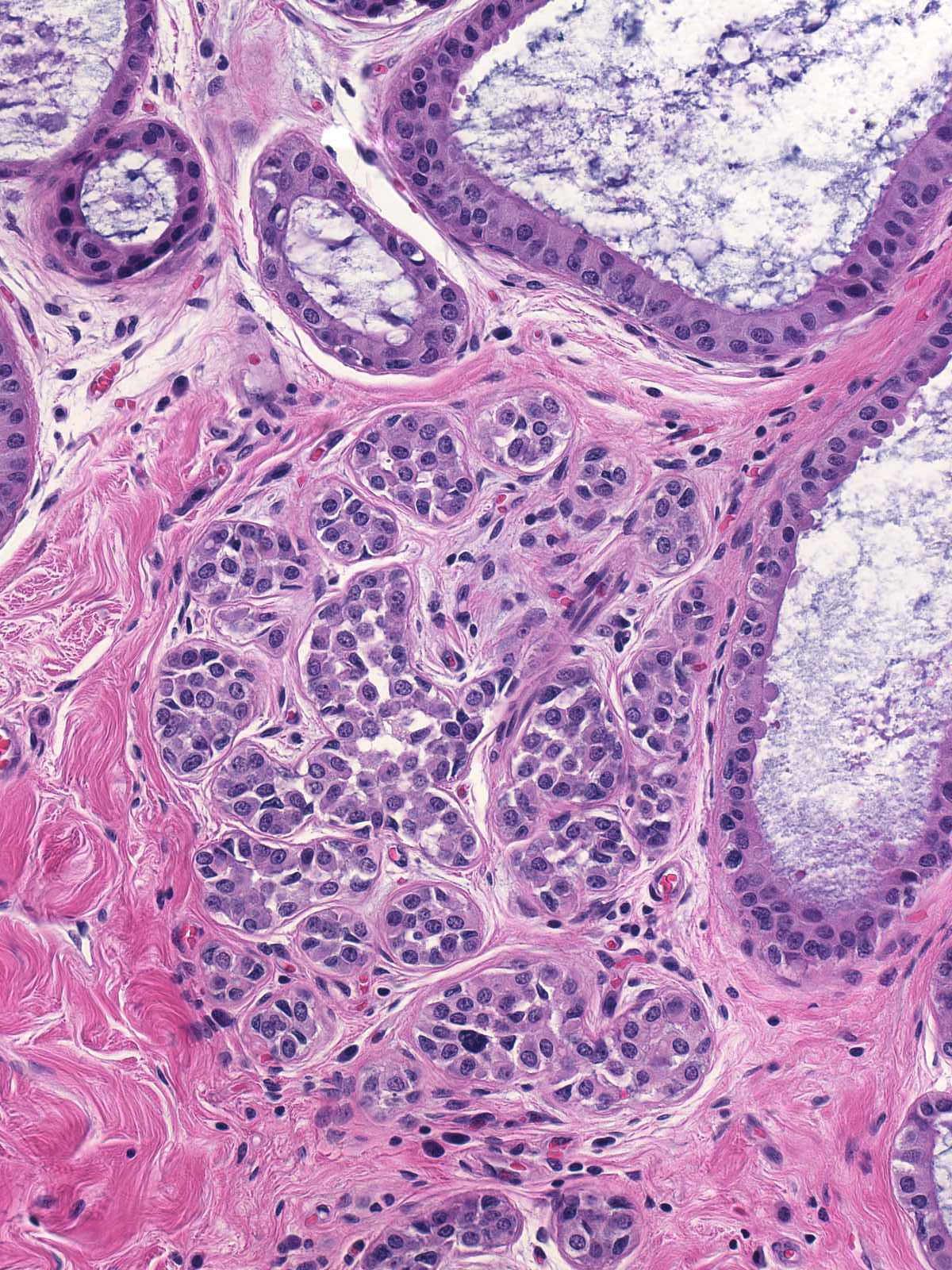
Flat atypia frequently coexists with lobular neoplasia and tubular carcinoma. Pathologists refer to this troika as the Rosen triad. Detection of any component of this group should prompt a careful search for the remaining members of the triad.
 |
 |
| FEA and LCIS |
FEA and tubular carcinoma |
Breast Pathology
