General
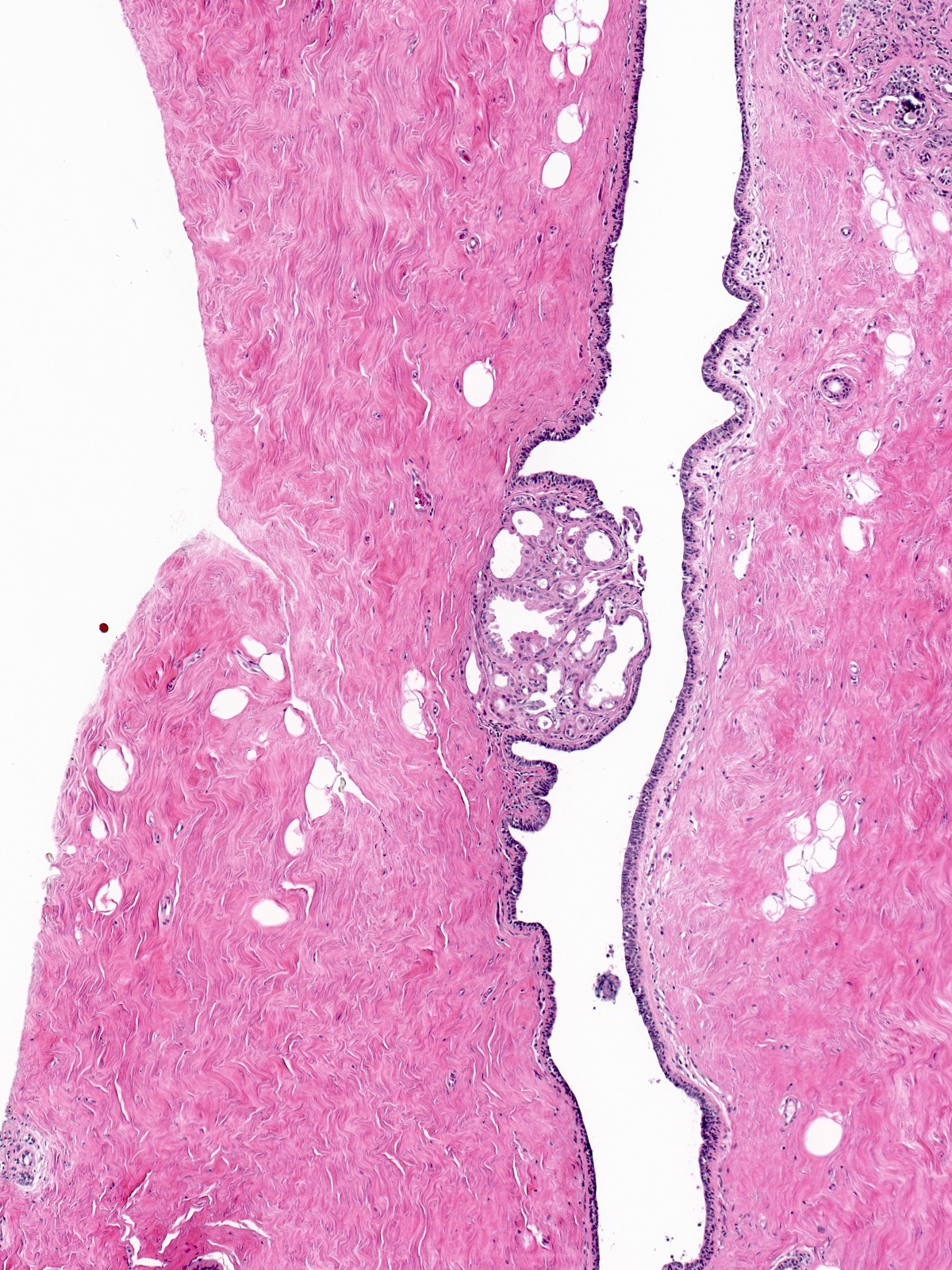
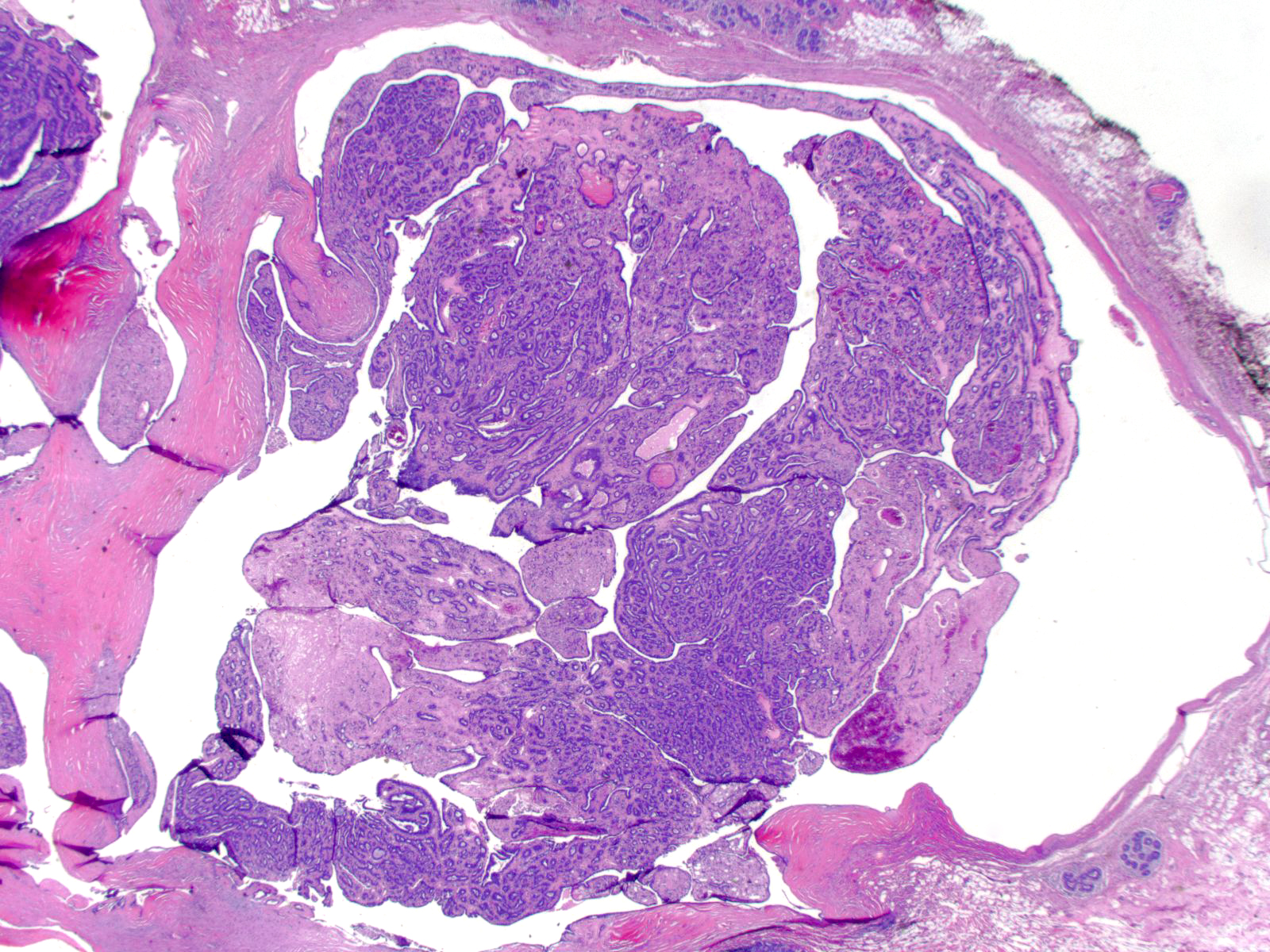
This 1928 image shows the gross appearance of a central papilloma, which, along with the lactiferous sinus in which it grew, prolapsed through the nipple orifice.
- Definition: A papilloma is a benign tumor composed of glands and stroma growing in an arborizing pattern within a duct.
- Clinical Significance: Papillomas can arise at any point in the ductal system, but they show a predilection for its extremes: the large ducts beneath the nipple, and the terminal ductules at the periphery of the breast. Central, large duct papillomas usually arise singly and come to attention because of a blood-stained discharge from the nipple or a palpable mass. Peripheral, small duct papillomas occur in clusters and usually form small, nonpalpable nodules that are revealed by imaging. Patients with multiple papillomas have an increased risk for the development of invasive carcinoma. When a core biopsy reveals a papilloma, surgeons usually carry out an excision of the targeted site to exclude the presence of a more serious lesion such as carcinoma in‑situ or invasive carcinoma.
- Gross Findings: Papillomas grow as well defined, round, bosselated tan nodules protruding into dilated ducts or cavities. Accumulation of fluid can enlarge the duct to create a partly cystic mass. Infarction, hemorrhage, and scarring frequently occur and can alter the appearance in the expected ways.
- Microscopic Findings: Papillomas consist of glandular tissue growing on an arborizing stromal skeleton. The glandular tissue looks like that seen in small ducts and terminal duct lobular units. The stroma has the characteristics of nonspecialized stroma.
- Differential Diagnosis: Papillary carcinoma (delicate supportive stroma, lacks myoepithelial cells), adenomyoepithelioma (An adenomyoepithelioma is a benign tumor situated in the stroma and composed of glands and tubules in a collagenous matrix. The glandular elements consist of normally layered luminal and myoepithelial cells. Certain pathologists believe that adenomyoepitheliomas represent a variety of papilloma.)
- Discussion: Large duct papillomas and small duct papillomas have similar microscopic features and can undergo the same pathologic changes.
 |
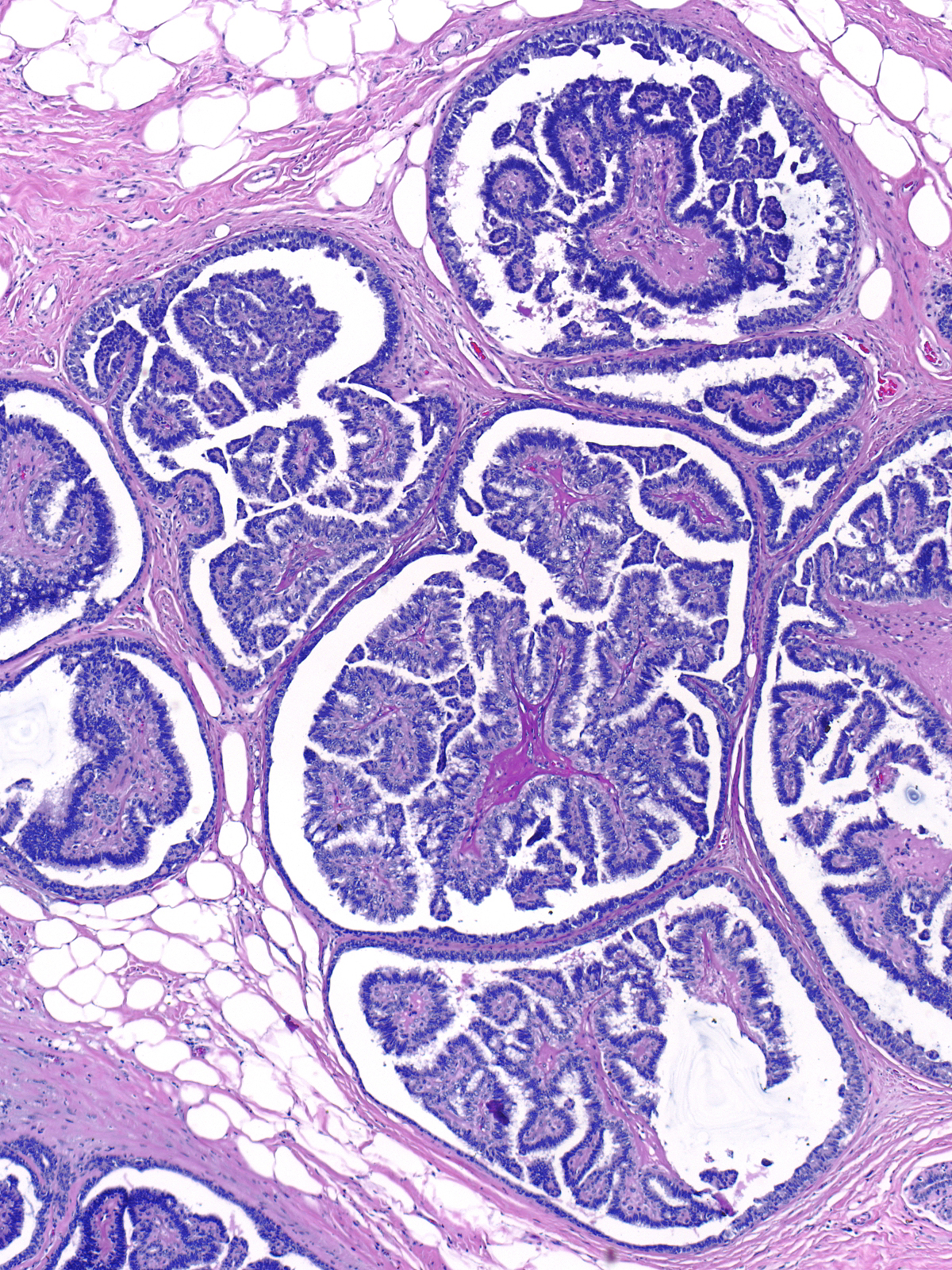 |
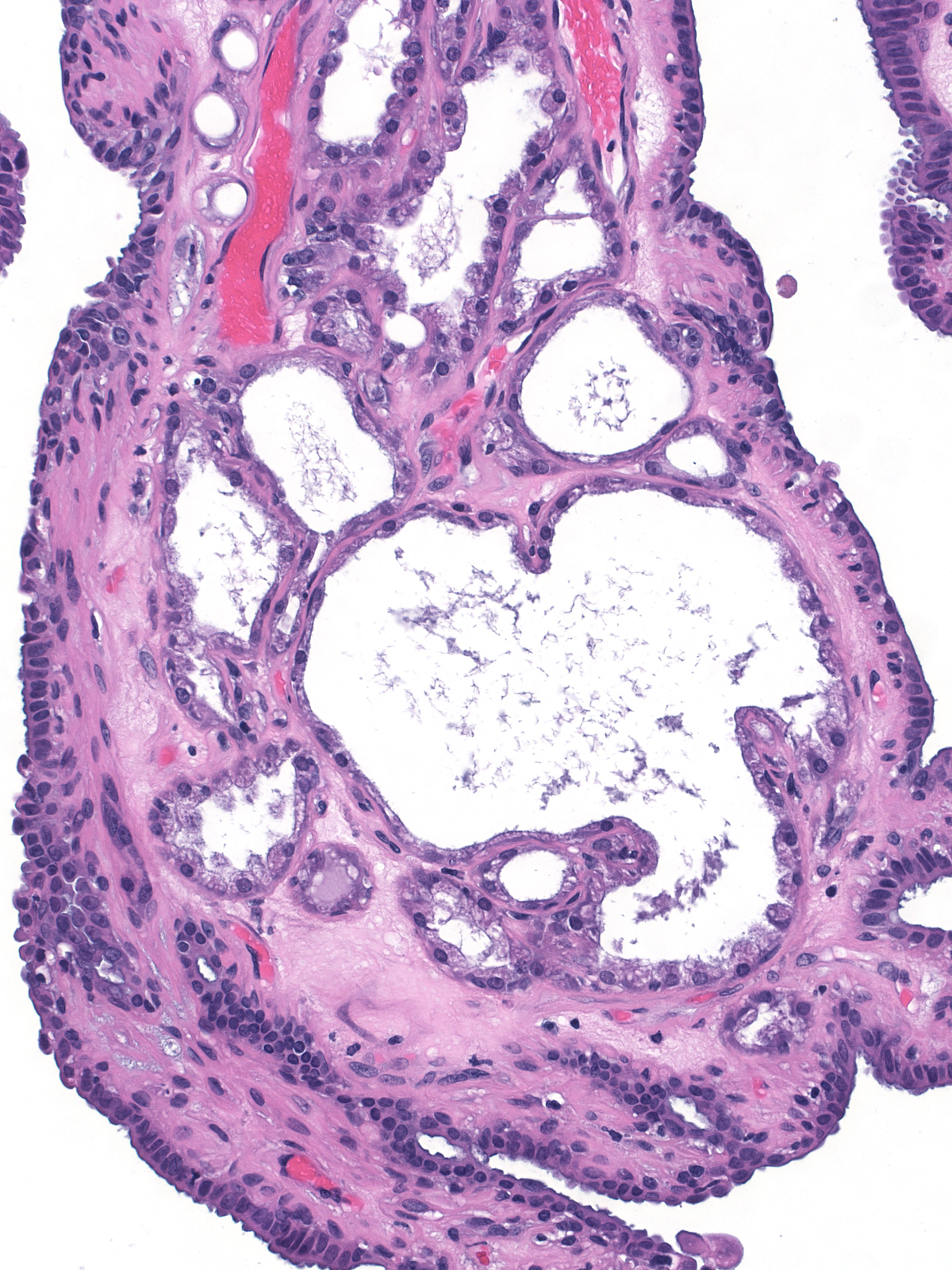
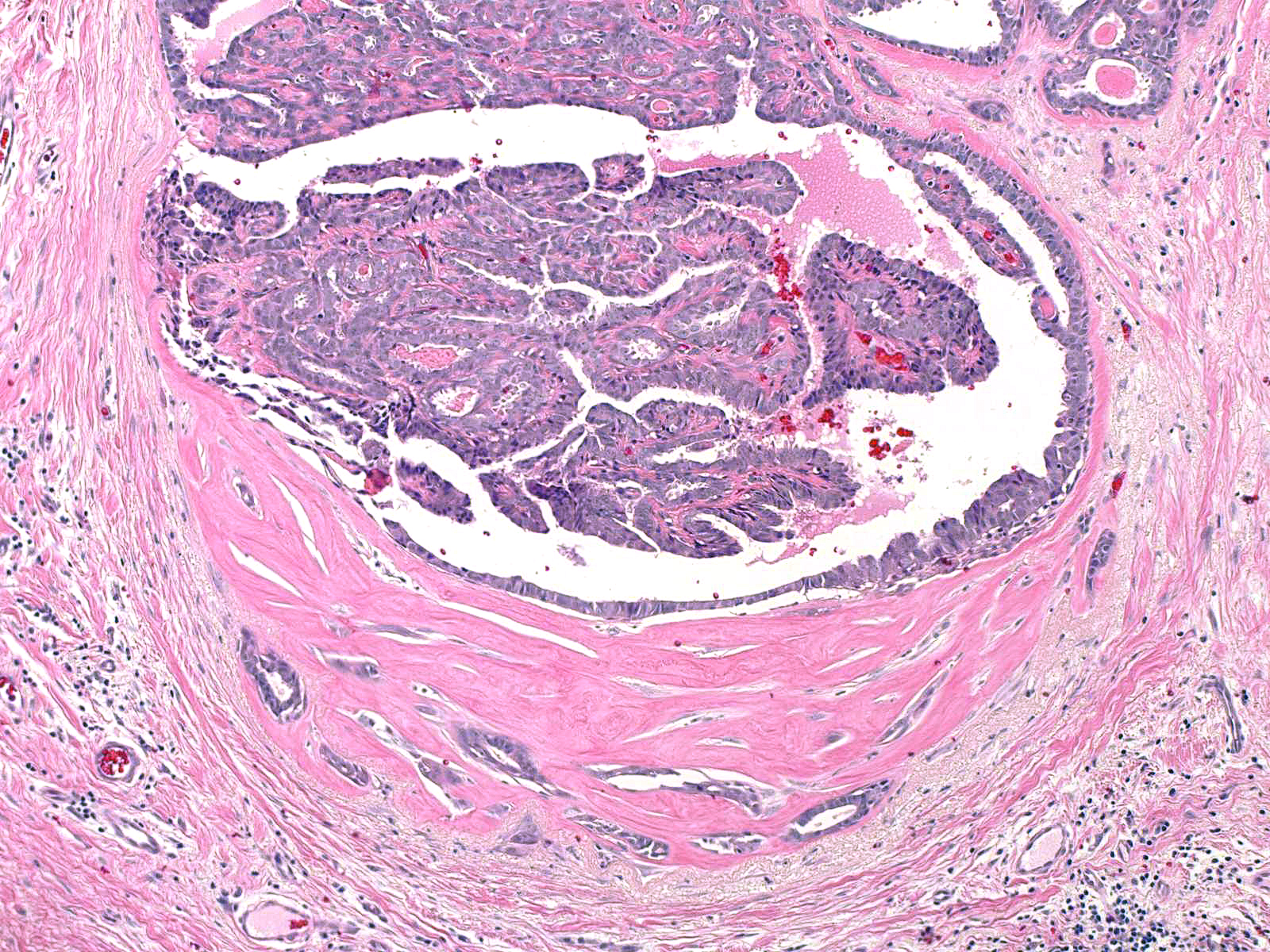
| A large, solitary papilloma involving a large duct |
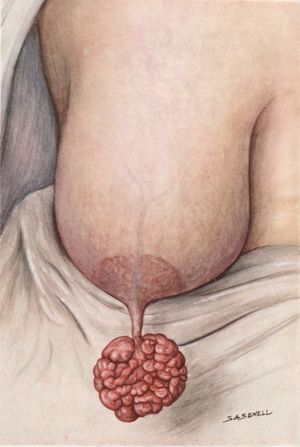
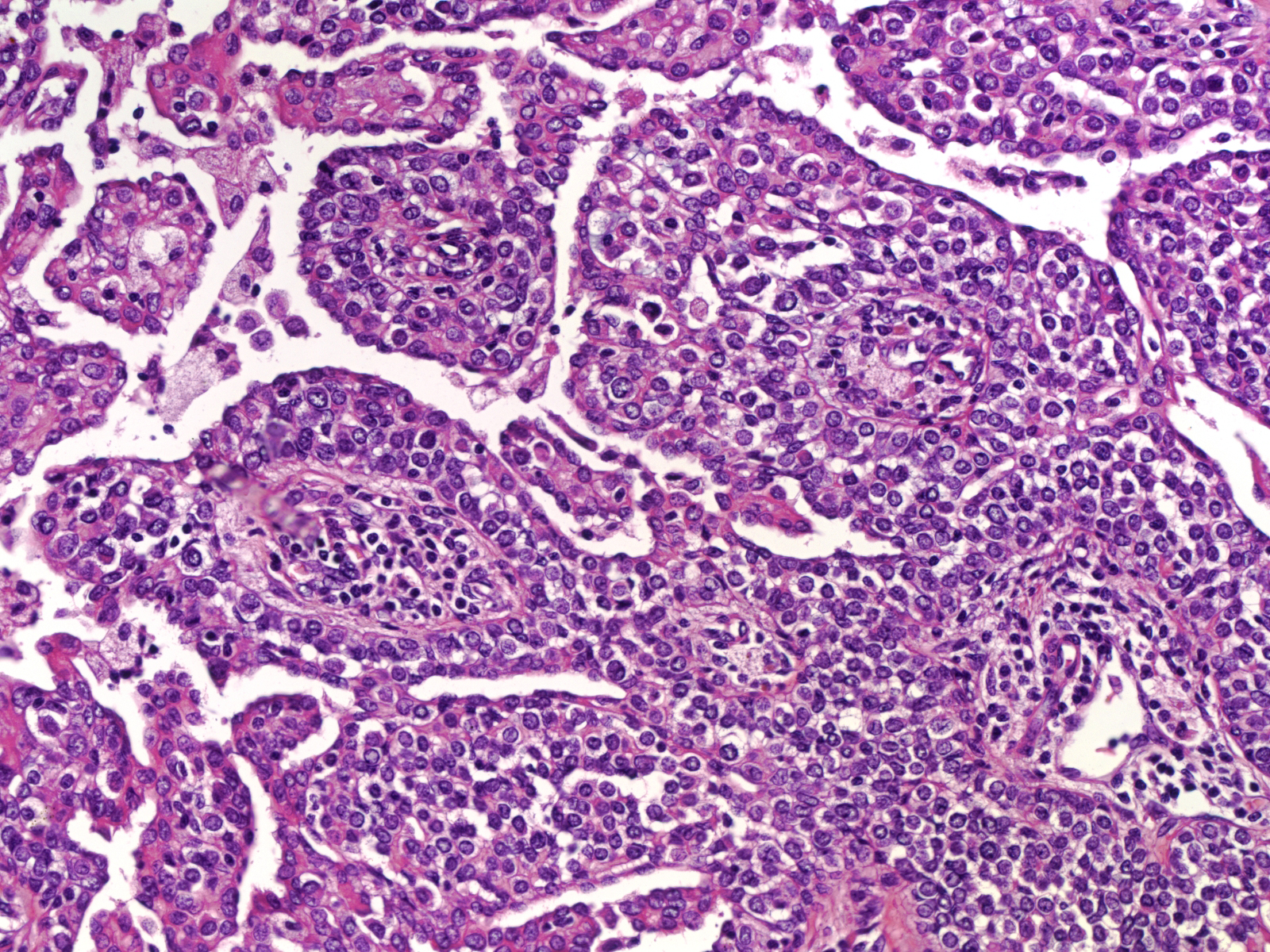
Smaller papillomas involving peripheral terminal ducts |
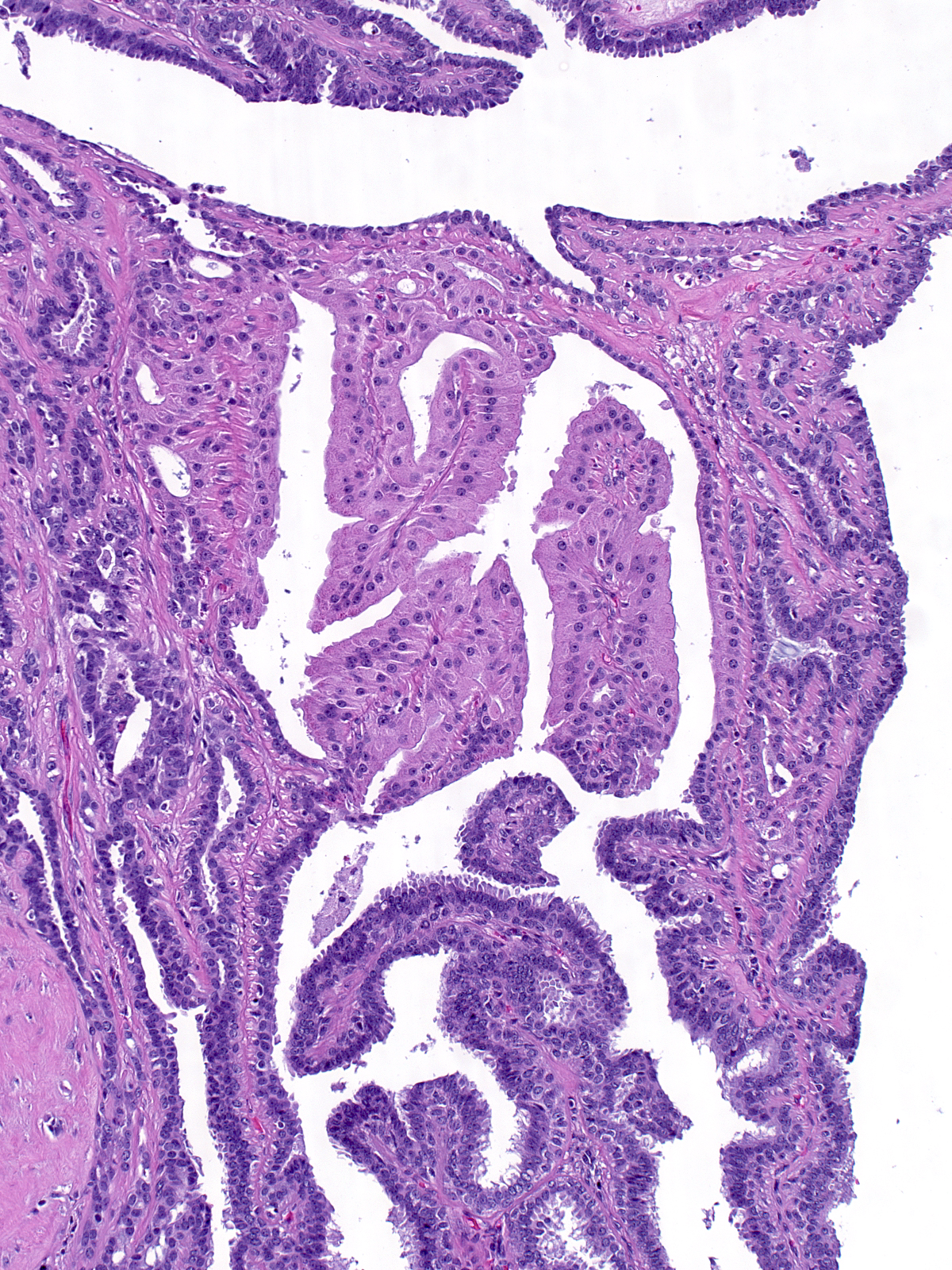
Architecture of Papillomas
| Papillomas consist of a small number of fronds, which exhibit blunt, polygonal shapes and appear to fit together. |
 |
|
|
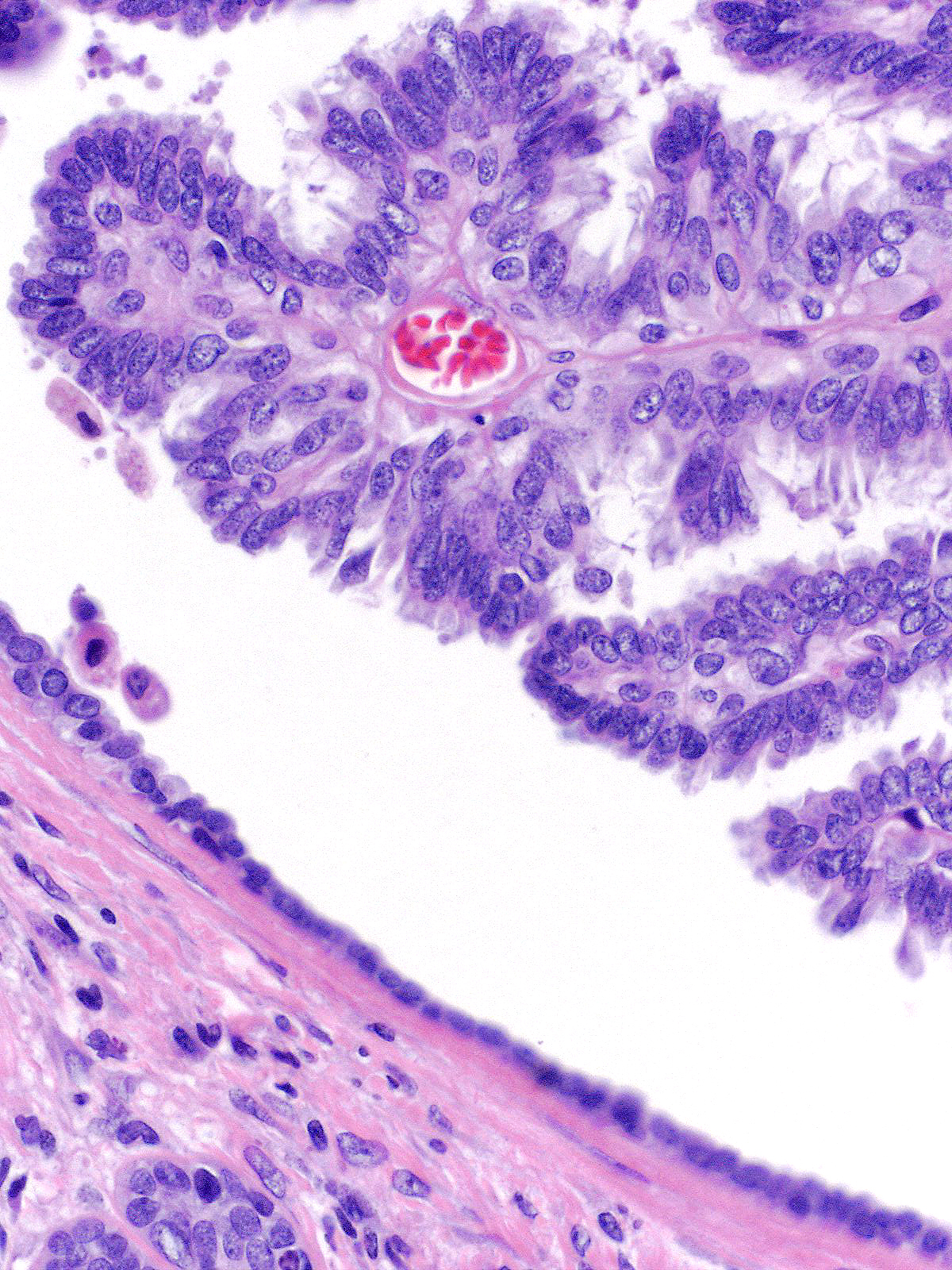
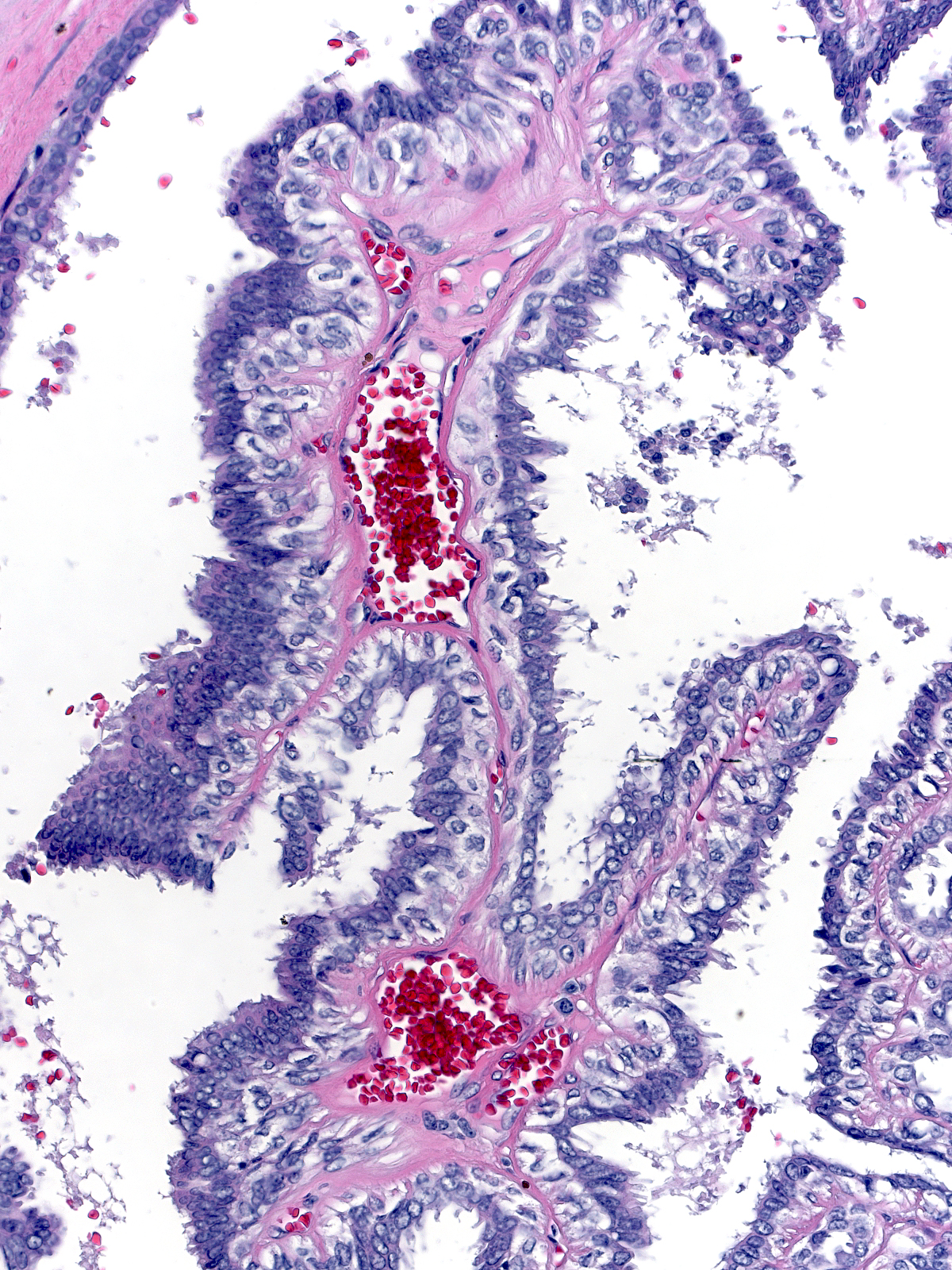
The fronds have substantial amounts of stroma and an epithelium composed of both luminal and myoepithelial cells.
Benign Alterations
The luminal cells, myoepithelial cells, and stroma of papillomas can each undergo benign alterations. The luminal cells frequently display apocrine change or, uncommonly, pregnancy-like change.
 |
 |
| Apocrine change |
Pregnancy-like change |
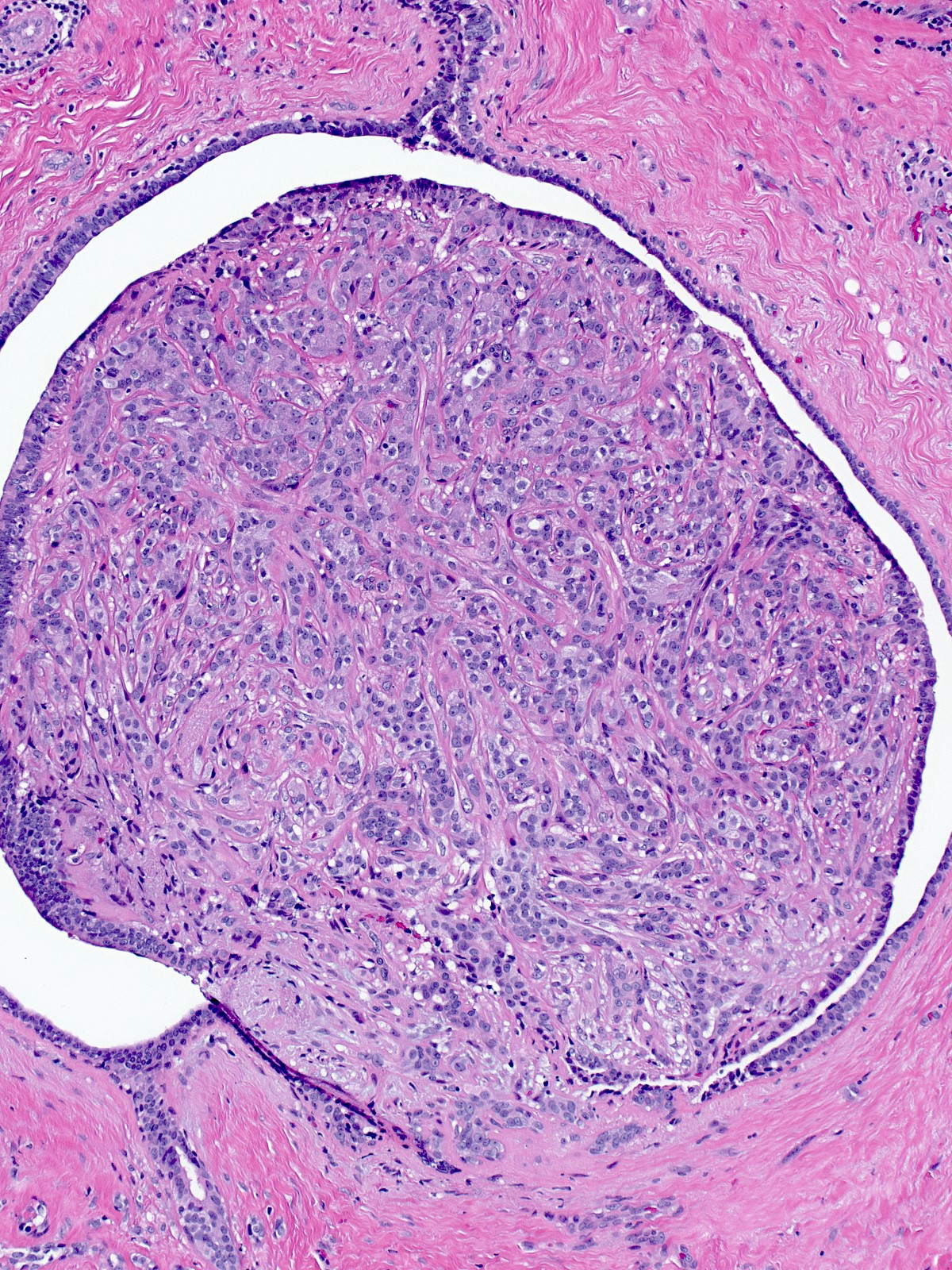
The myoepithelial cells can appear prominent or hyperplastic.
 |
 |
| Prominent myoepithelial cells |
Hyperplastic myoepithelial cells showing polygonal shapes |
The hyperplastic myoepithelial cells can assume polygonal shapes, as seen above, or spindly shapes, as seen here.
 |
 |
| Spindled myoepithelial cells |
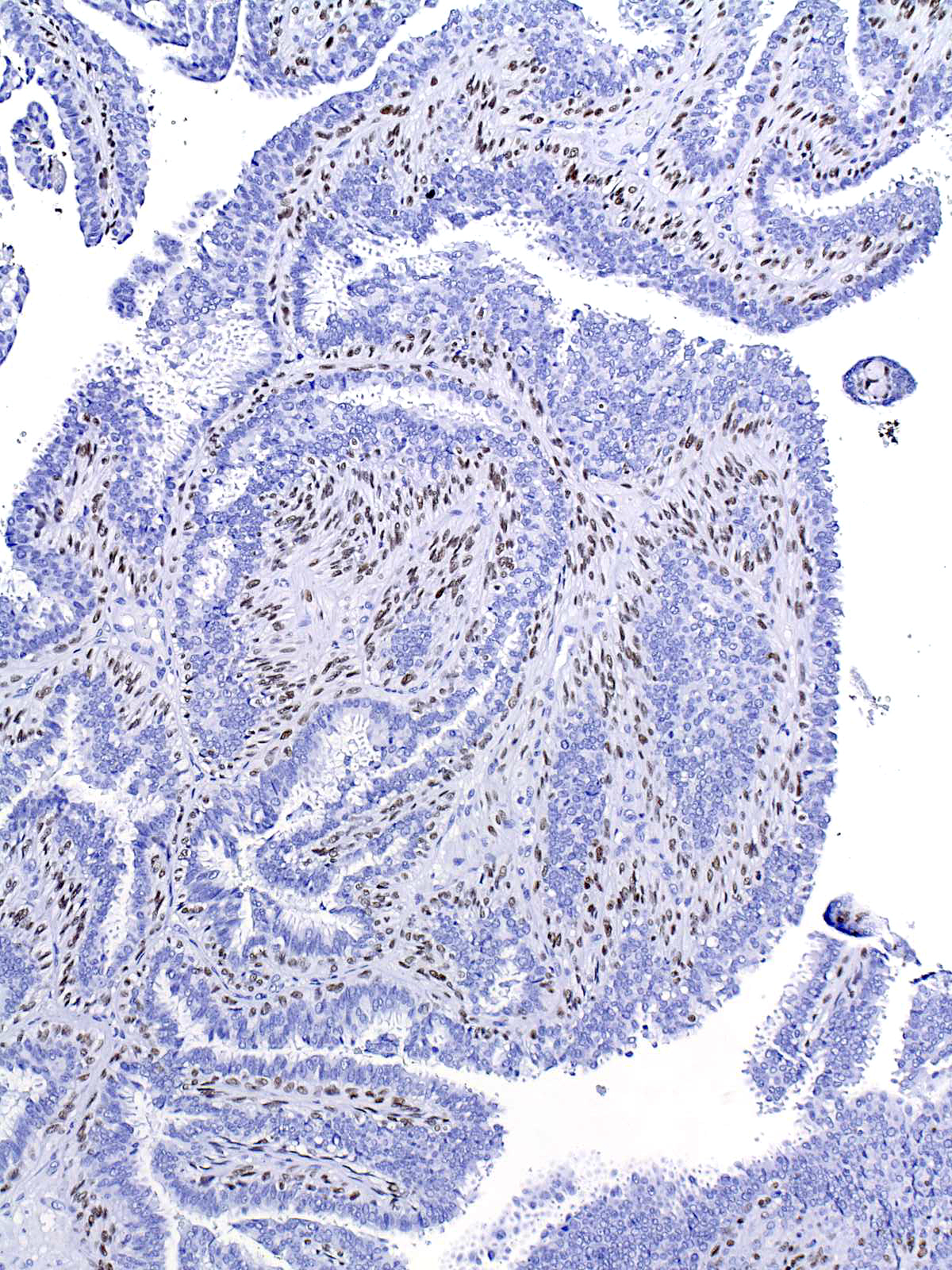
A stain for p63 |
| The myoepithelial cells within papillomas frequently give rise to foci of collagenous spherulosis. |
 |
|
|
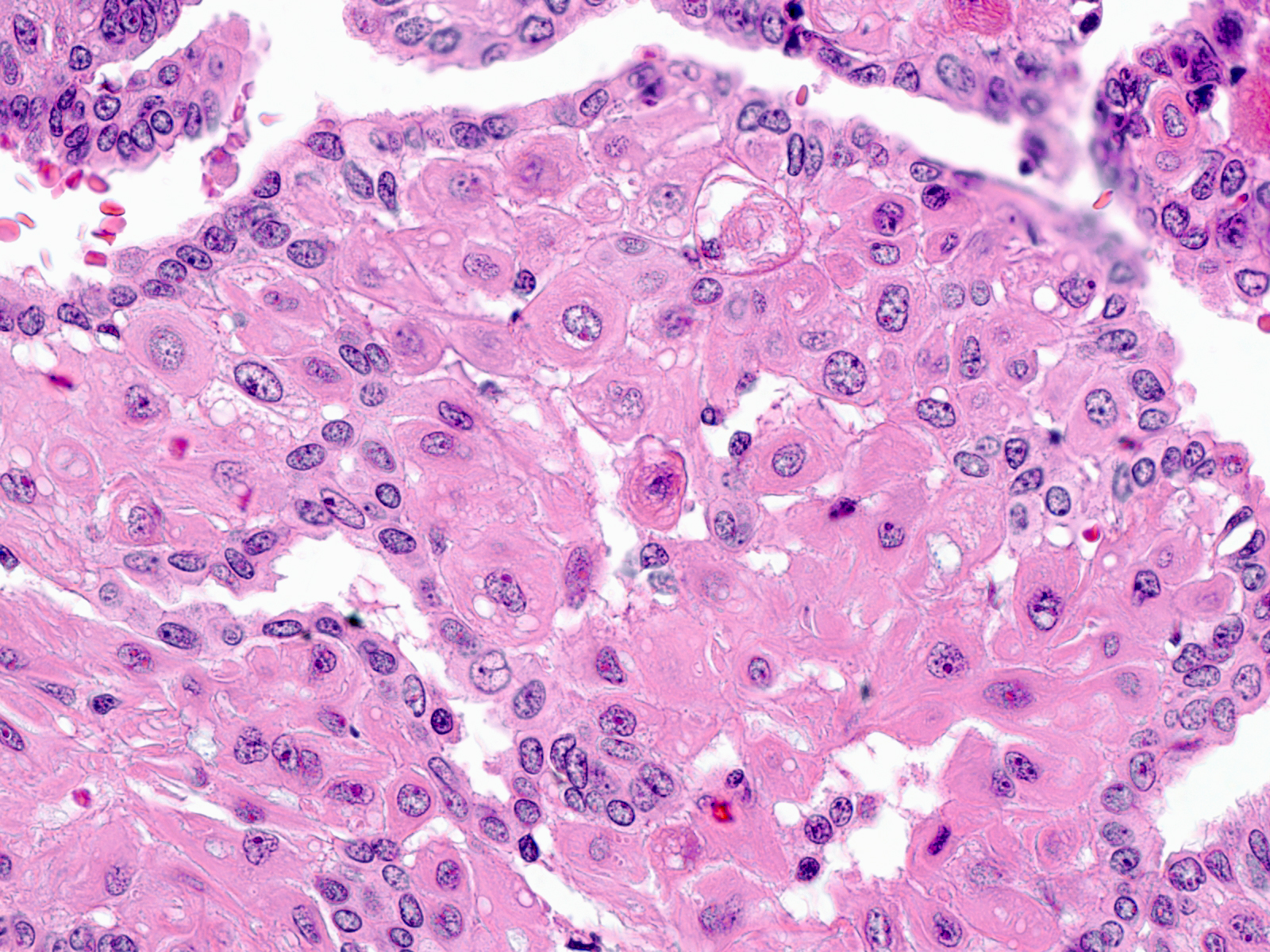
| Complicating matters, the myoepithelial cells can develop apocrine-like changes. These large cells have large nuclei, vesicular chromatin, prominent nucleoli, and abundant, eosinophilic and vacuolated cytoplasm. |
 |
|
|
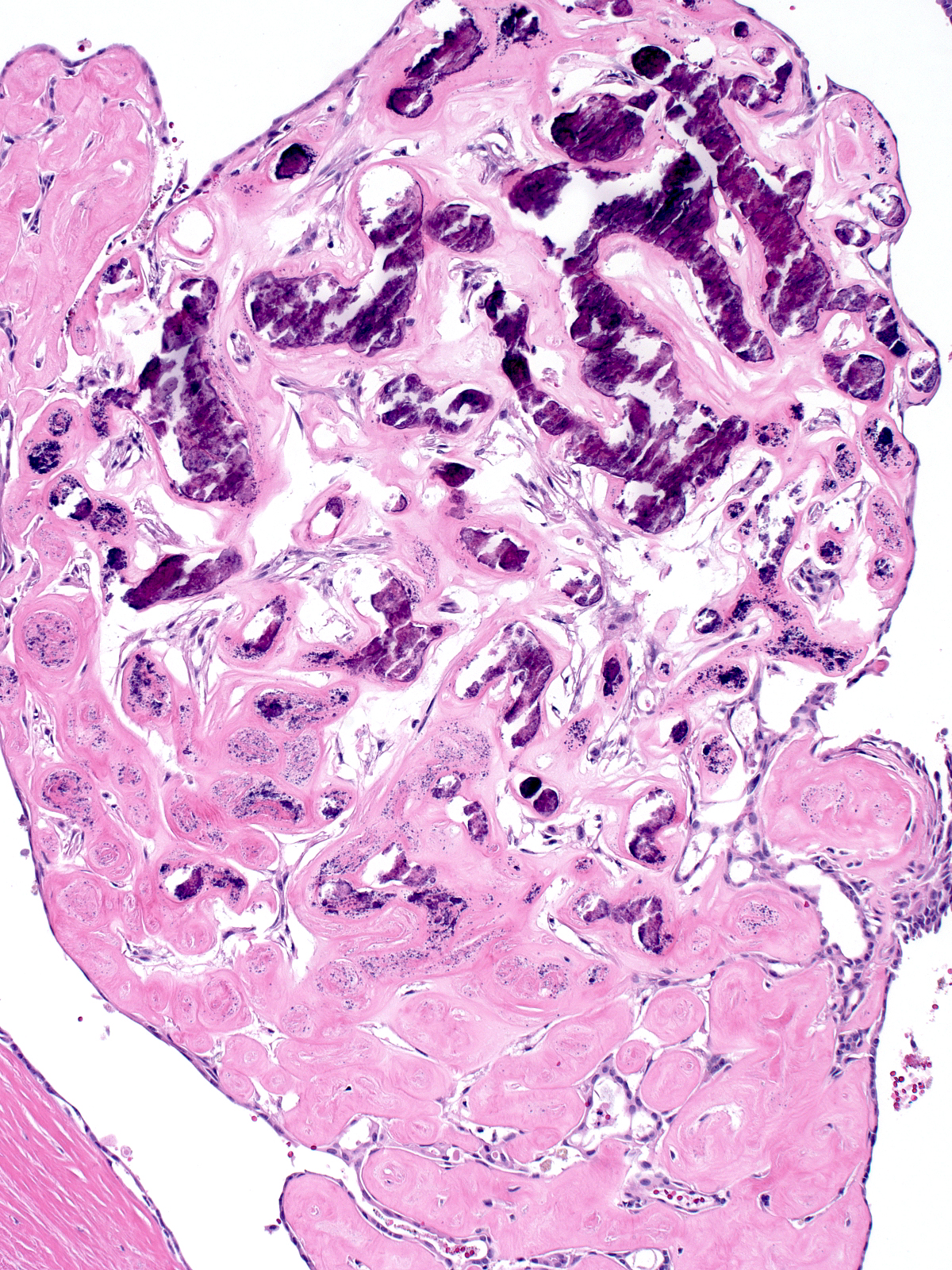
Regions of the stroma often become sclerotic and can calcify.
| When the sclerosis extends into the surrounding tissue, pathologists often classify the tumor as a sclerosing papilloma. |
 |
|
|
| The sclerosis can entrap nearby glands and produce an appearance that superficially resembles invasive carcinoma. |
 |
|
|
Superimposed Epithelial Proliferations
Epithelial proliferations can involve papillomas in two locations: on the surface of the fronds, and within the stalk of the papilloma. One analyzes proliferations on the surface of the fronds in the way that one does for proliferations affecting ducts without papillomas. The most common epithelial proliferations involving papillomas include: usual ductal hyperplasia, atypical ductal hyperplasia, ductal carcinoma in-situ, and lobular neoplasia. Each type of proliferation displays its characteristic cytological and architectural features.
 |
 |
| Involvement by UDH |
Involvement by ADH |
 |
 |
| Involvement by DCIS |
Involvement by LCIS |
| Occasionally, superficial hyperplastic cells also exhibit a set of changes characteristic of hyperplastic cells involving papillomas and considered degenerative: binucleation, irregularity of the nuclear contours, prominence of the nucleoli, and the accumulation of abundant, eosinophilic, and often vacuolated cytoplasm. |
 |
|
|
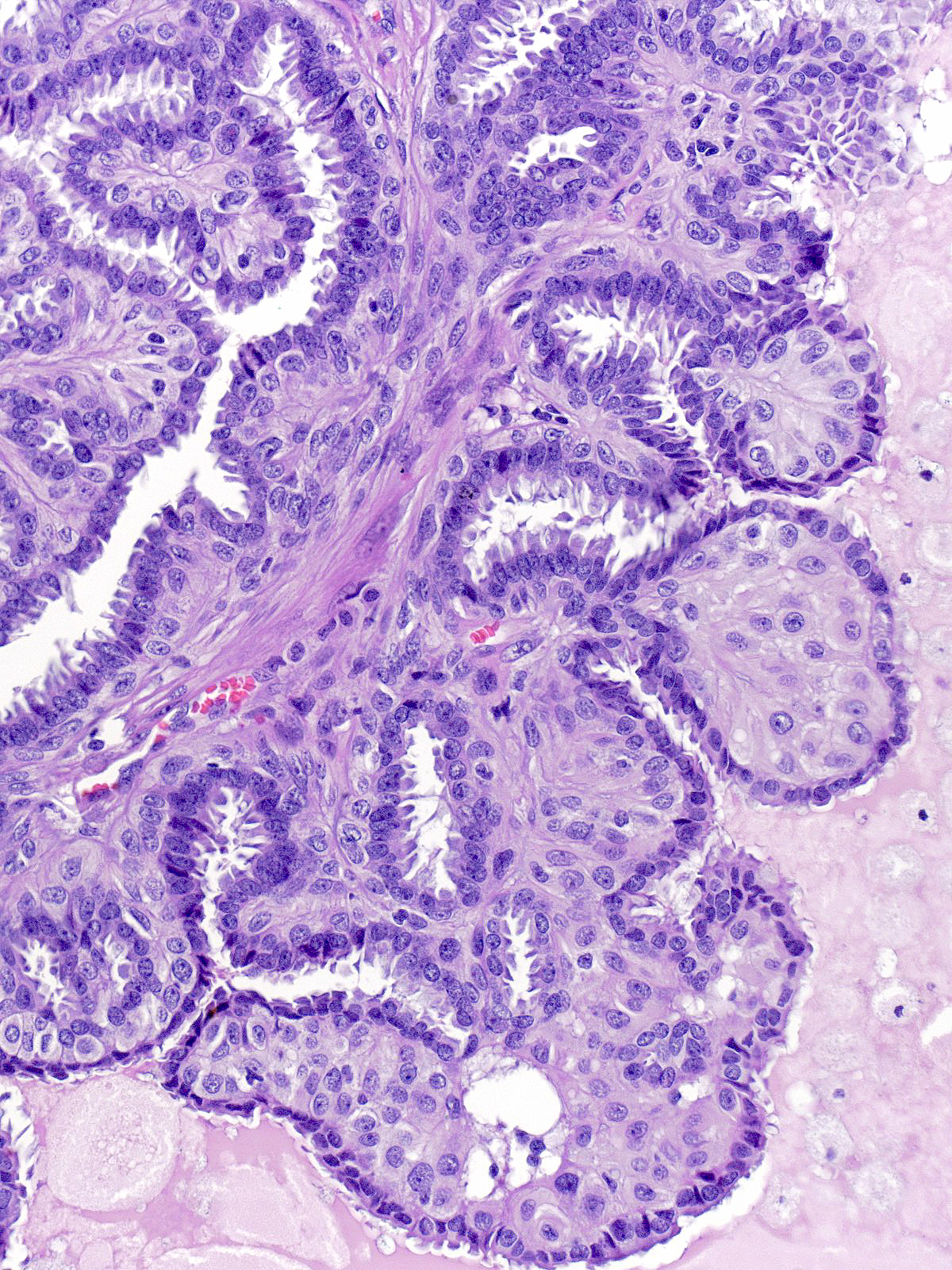
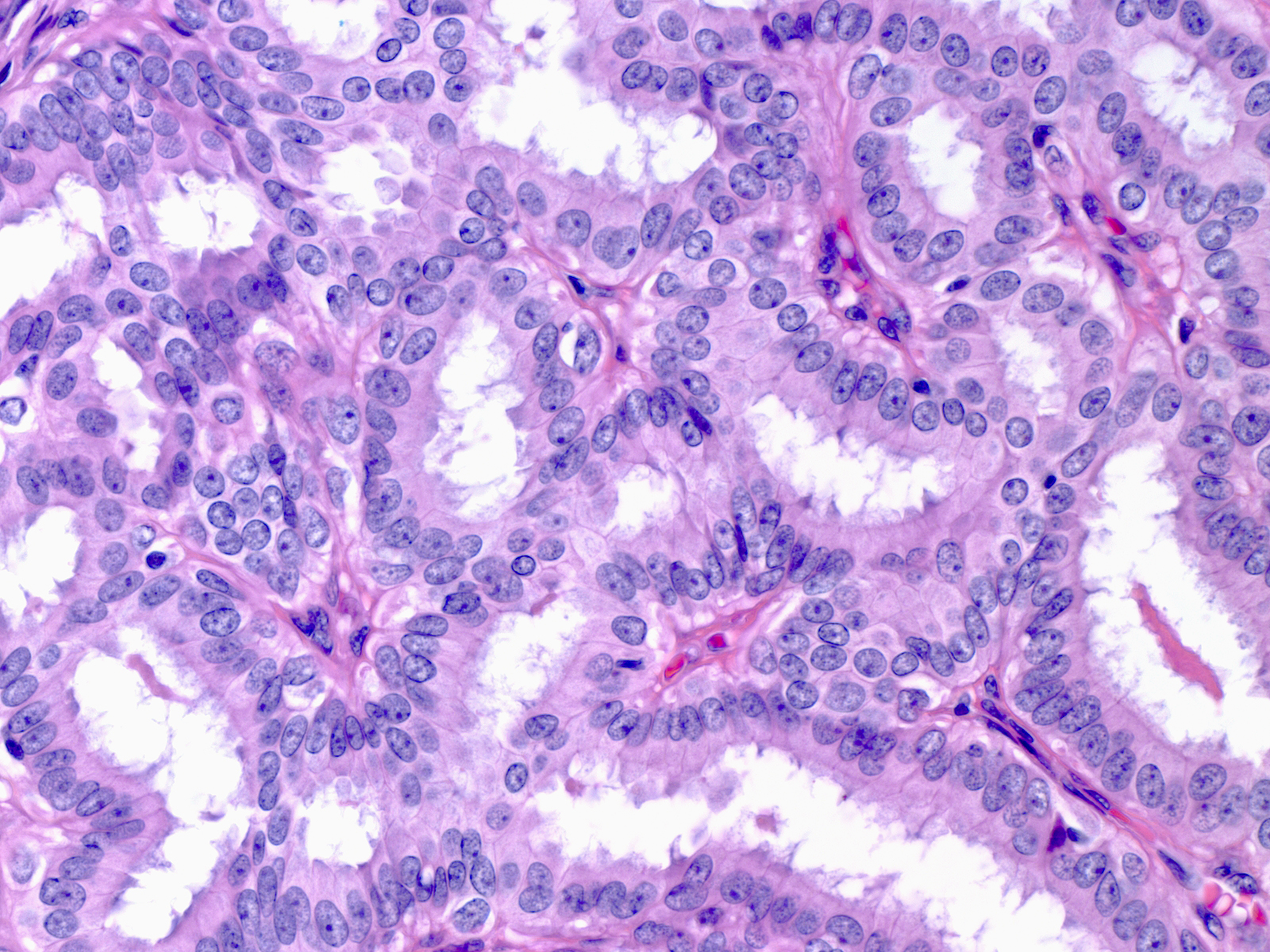
| Epithelial proliferations within the stalk of a papilloma usually take the form of an adenosis-like multiplication of closely packed acini referred to as the complex glandular pattern. One could easily mistake this appearance for cribriform ductal carcinoma in-situ if one failed to appreciate the basement membranes and delicate fibrovascular stroma surrounding each gland. |
 |
|
|
Complications Affecting Papillomas
| Infarction of a frond of a papilloma usually accounts for the complaint of a bloody nipple discharge.14-25 Infarcted_frond.jpg |
|
|
|
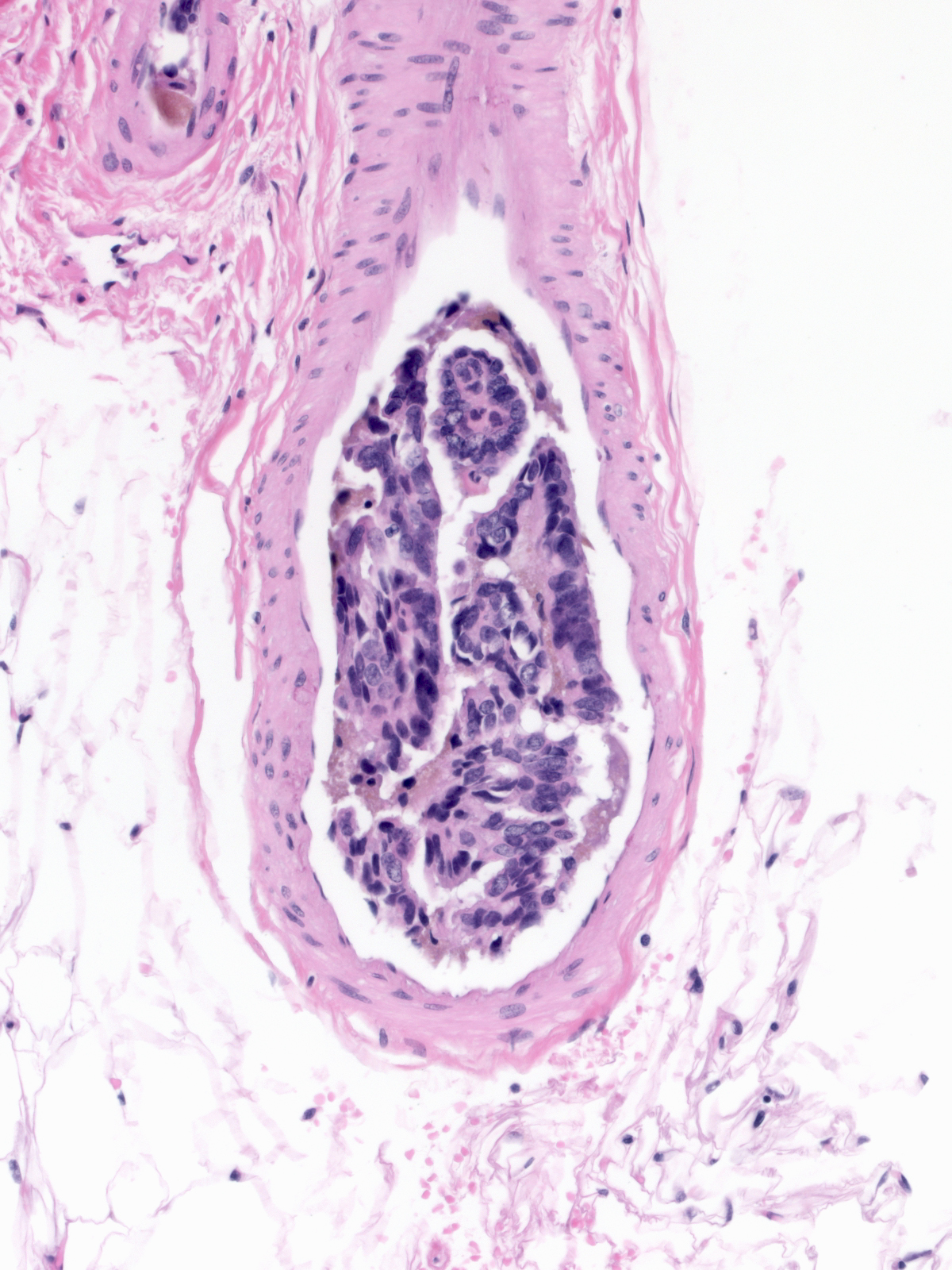
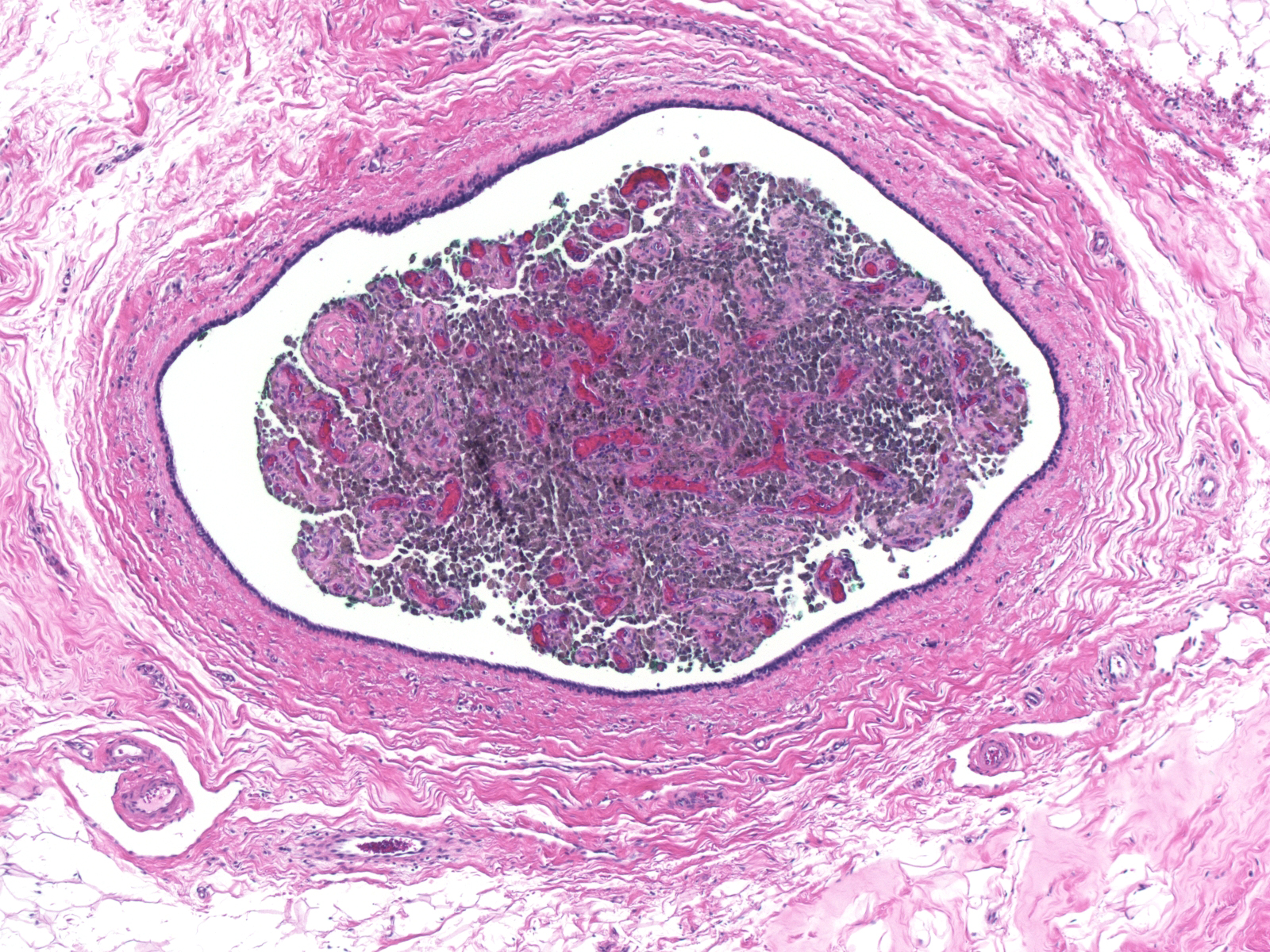
| Occasionally, the entire papilloma undergoes infarction. |
 |
|
|
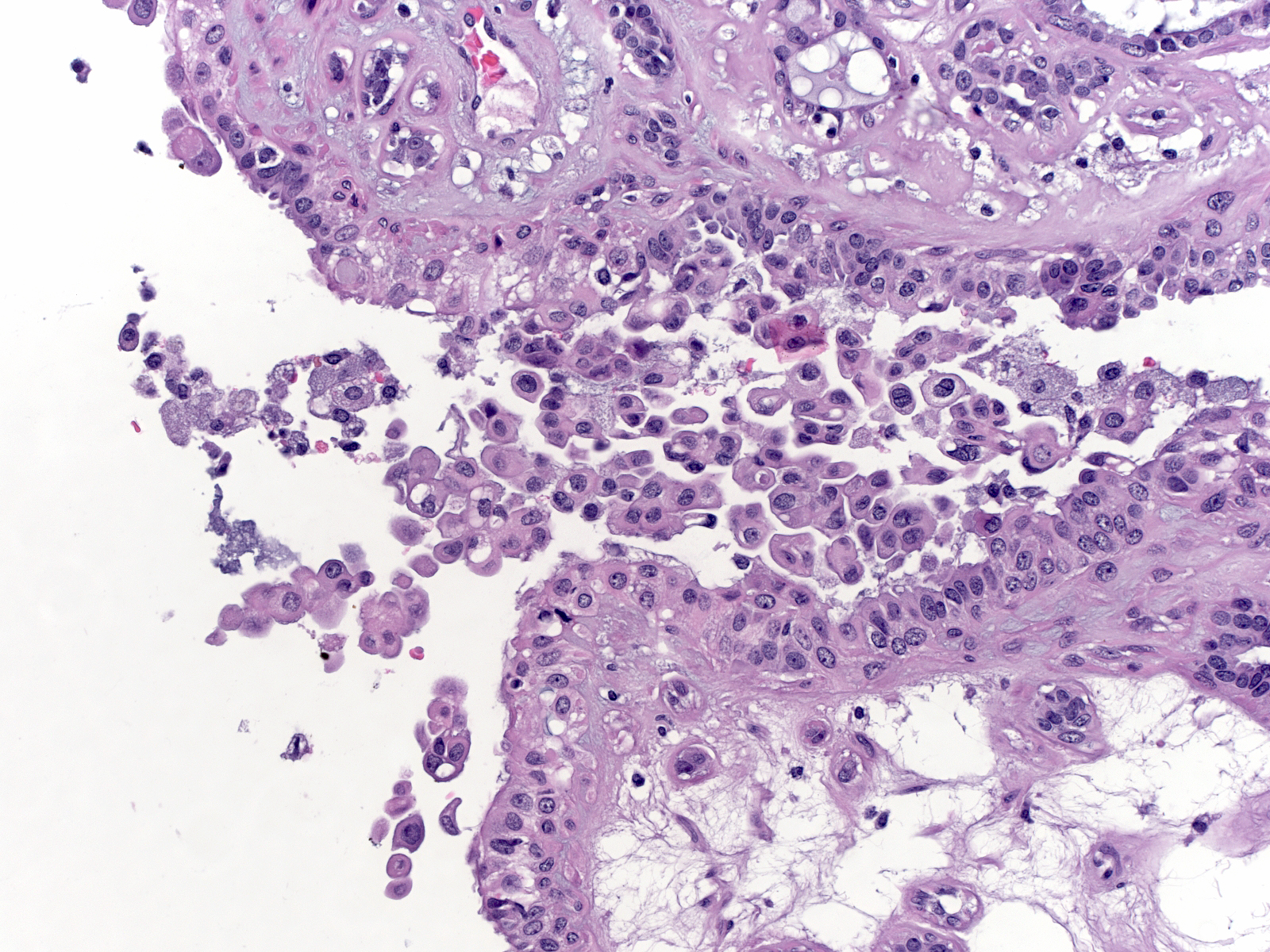
| A core biopsy of a papilloma harboring florid ductal hyperplasia can leave clusters of hyperplastic epithelial cells in the needle track. |
 |
|
|
These displaced cells and papilloma fragments can make their way into lymphatic vessels, veins, and axillary lymph nodes.
Pathogenesis
The pathogenesis of papillomas is unknown. Papillomas arising in large ducts may develop when a small portion of lobular tissue (including lobular stroma) becomes entrapped within the wall of a duct. Ingrowth of ductule-like structures could give the mass a papillary configuration.
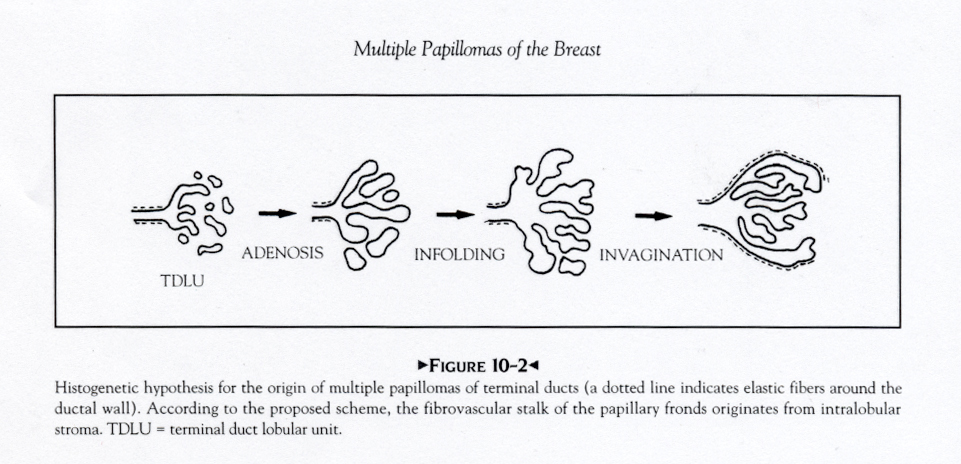
| Small duct papillomas most likely arise through a process called lobular unfolding. |
 |
|
|