|
Definition: Invasive lobular carcinoma (ILC) is an invasive mammary adenocarcinoma composed of dishesive, nonpolarized cells.
Clinical Significance: Invasive lobular carcinoma accounts for approximately 15% of invasive breast carcinomas in women; it occurs only very rarely in men. The carcinoma presents either as a mass or as an architectural abnormality detected by imaging.
Gross Findings: Invasive lobular carcinomas are often indistinct to the unaided eye but are otherwise similar to commonplace invasive breast carcinomas. They form irregular, ill-defined masses that feel firm or hard and are composed of white, tan, or pale yellow tissue that does not bulge from the cut surface. For additional description, see the invasive carcinoma section of the basic gross pathology page.
Microscopic Findings: Lobular carcinoma cells typically appear small and uniform, but uncommon examples display marked pleomorphism (see pleomorphic lobular carcinoma). Mitotic figures are typically difficult to find, necrosis does not occur in most cases, and one detects lymphovascular invasion only rarely. Typical cases are histological grade 2 and they stain for estrogen receptors.
Differential Diagnosis: Invasive ductal carcinoma growing in a dispersed pattern (more cohesive, evidence of polarization, membraneous E-cadherin), invasive ductal carcinoma with altered junctional complexes (cytoplasmic E-cadherin, focal subtle cohesion), sclerosing adenosis (lobulocentric, myoepithelial cells present, cells do not directly touch fat)
Discussion: Conventional invasive lobular carcinoma consists of dishesive cells with characteristic cytologic and architectural features. Because these features include only slight enlargement of the cells, minimal atypia, and dishesive growth patterns, ILC can be sneaky and difficult to detect. Careful attention to the features discussed below as well as the ample use of IHC stains will help to keep you out of hot water.
|
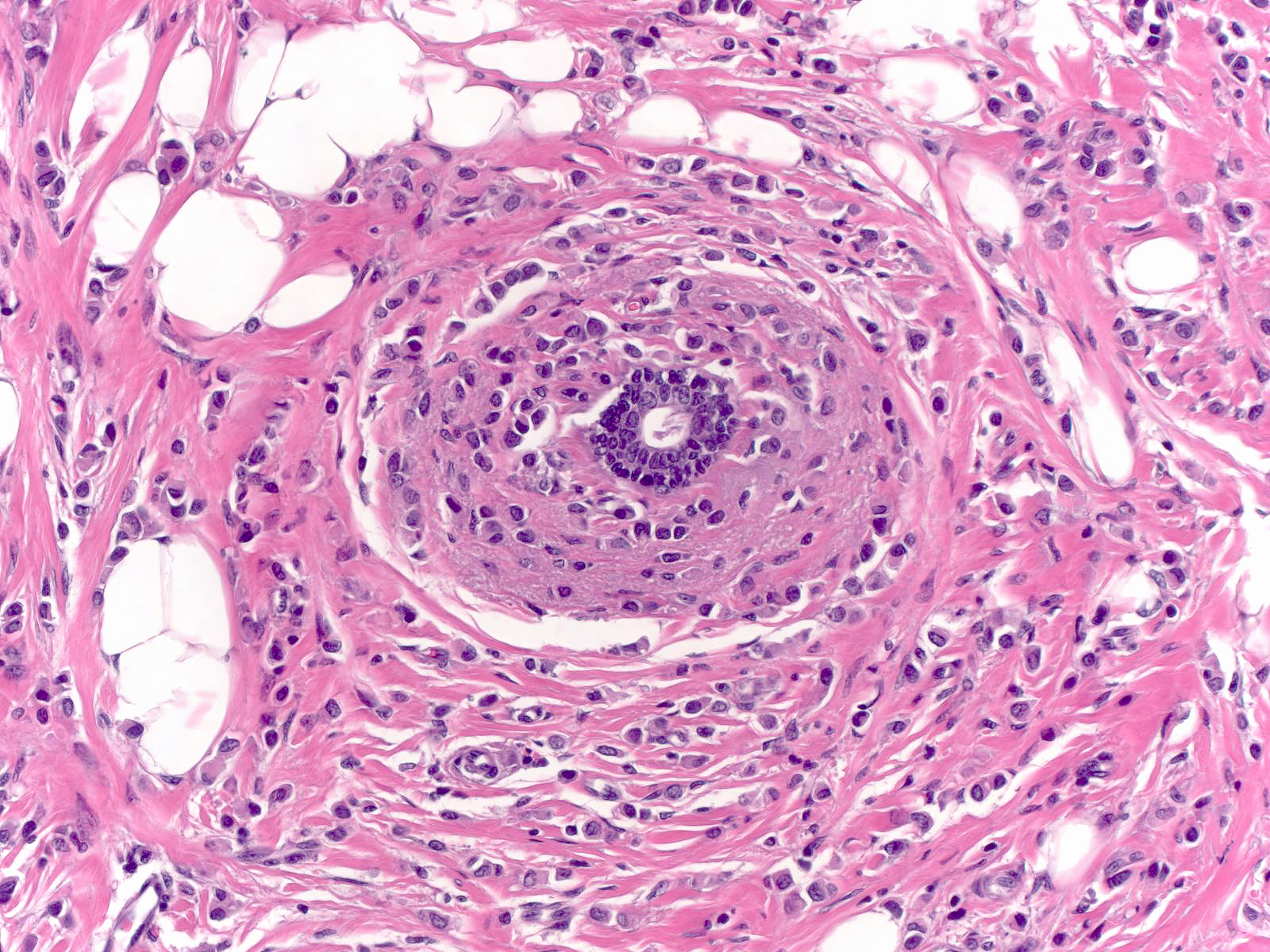
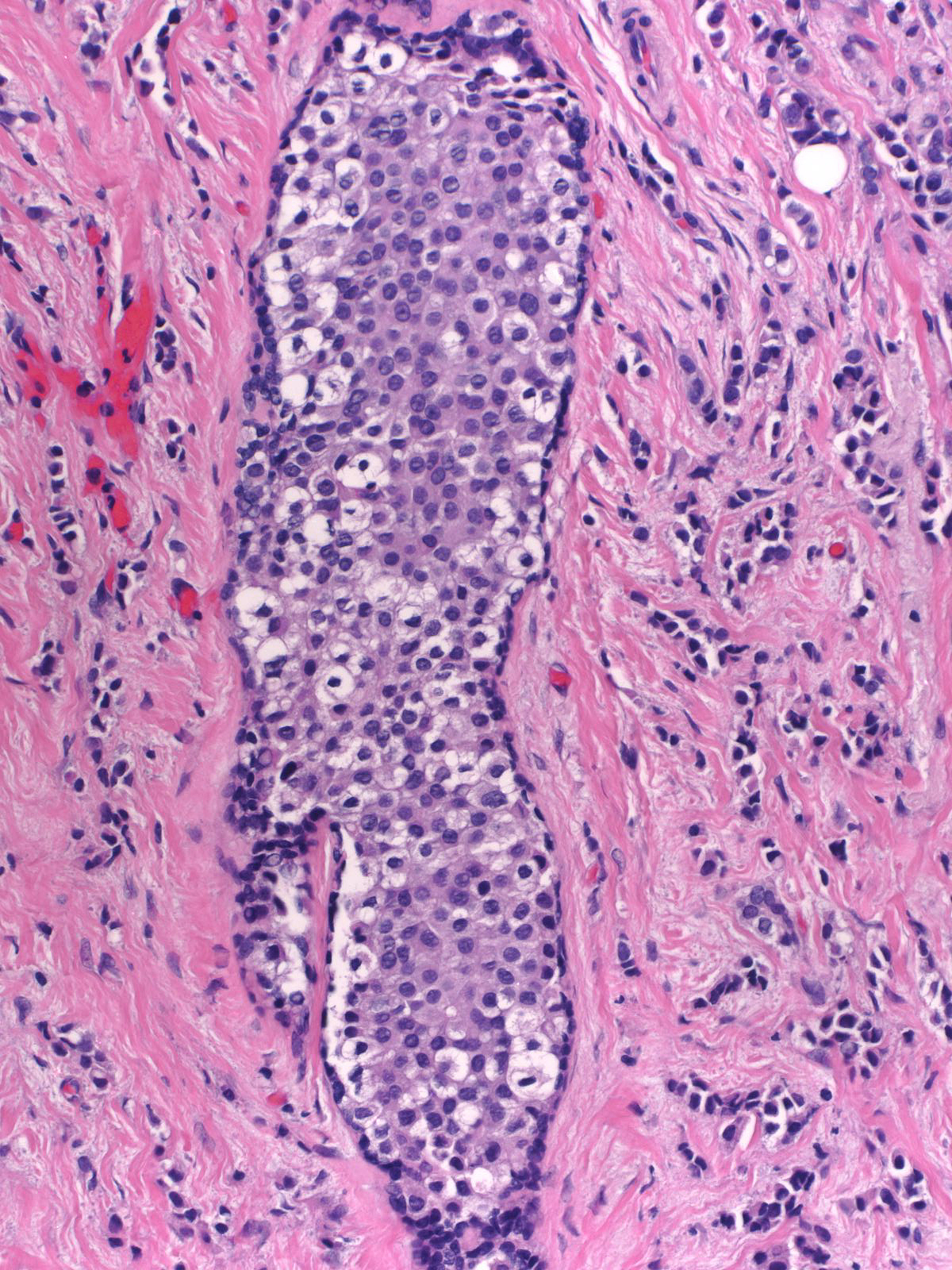
 These invasive lobular cells appear small and uniform, but they are still appreciably larger than the normal ductal cells in the center of the image. These invasive lobular cells appear small and uniform, but they are still appreciably larger than the normal ductal cells in the center of the image. |
Cytology
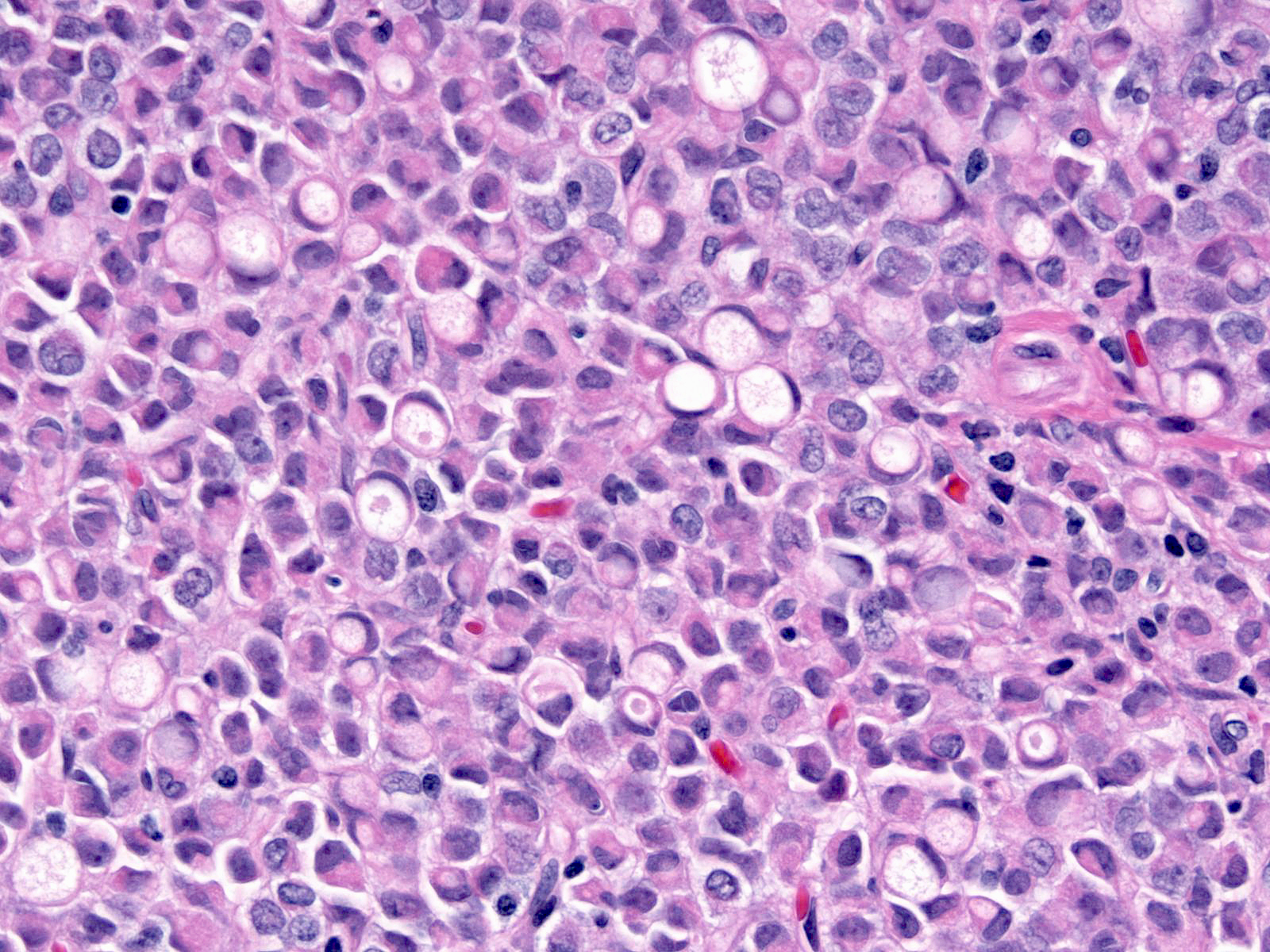
The chromatin of ILC cells usually looks pale and slightly granular (left), but it can also appear dark and dense (middle) or finely dispersed (right).
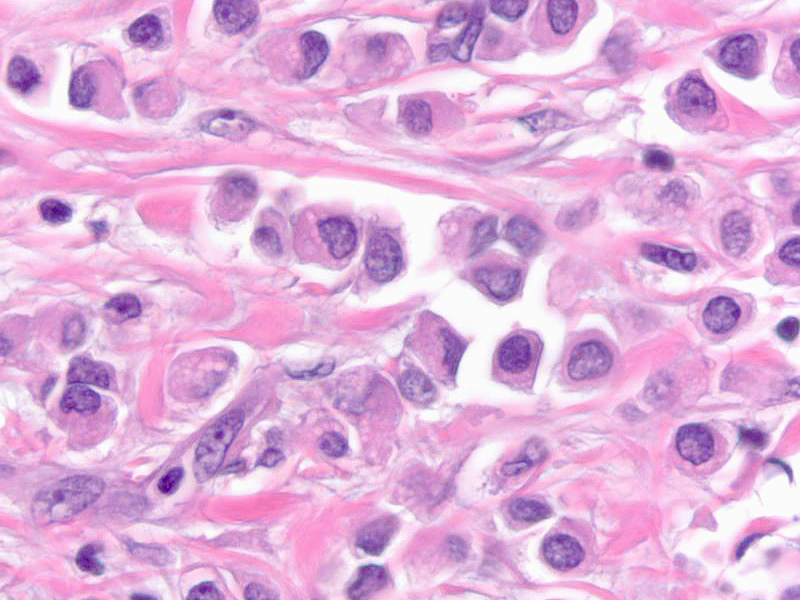
| The nuclei typically have irregular contours and inconspicuous nucleoli. The nuclei tend to sit at one edge of the cell and thereby create a plasmacytoid appearance. |
 |
|
|
| The cells contain scant eosinophilic cytoplasm, and the presence of miniscule mucin droplets gives it a foamy appearance. |
 |
|
|
| The cytoplasm sometimes contains large clear spaces. These spaces arise as a result of either the accumulation of abundant mucin or the formation of intracytoplasmic lumens. Pathologists refer to such cells as signet-ring cells regardless of the mechanism of their formation. |
 |
|
|
Patterns of Growth
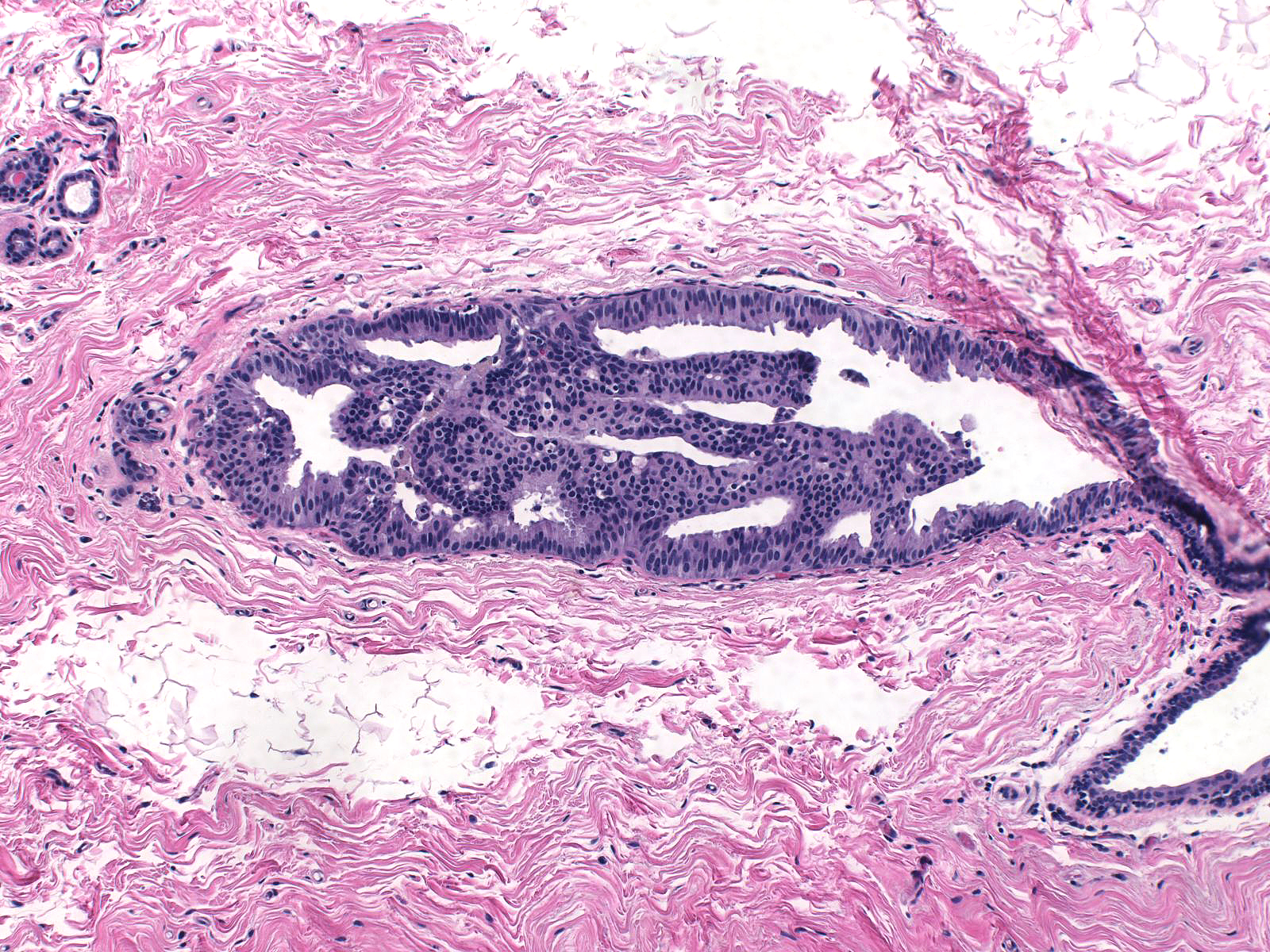
| Foci of invasion usually sit next to acini or ductules involved by lobular carcinoma in-situ. |
 |
|
|
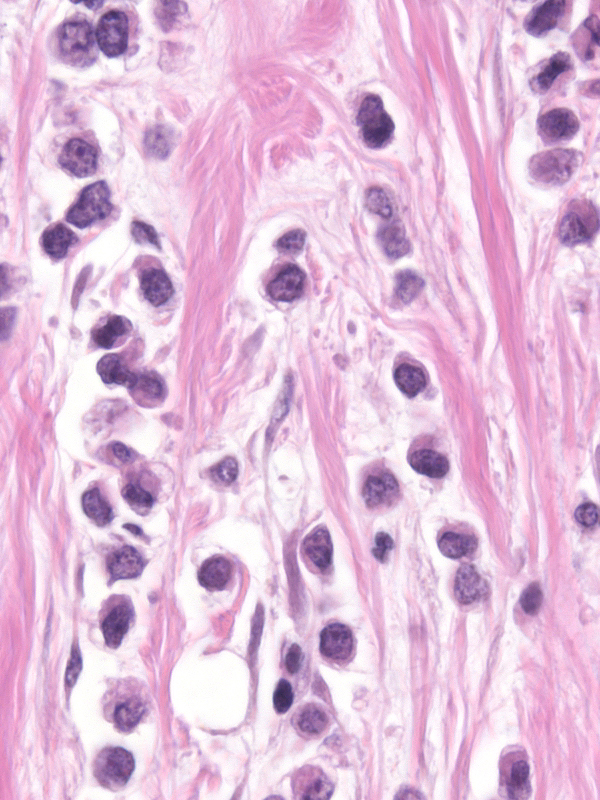
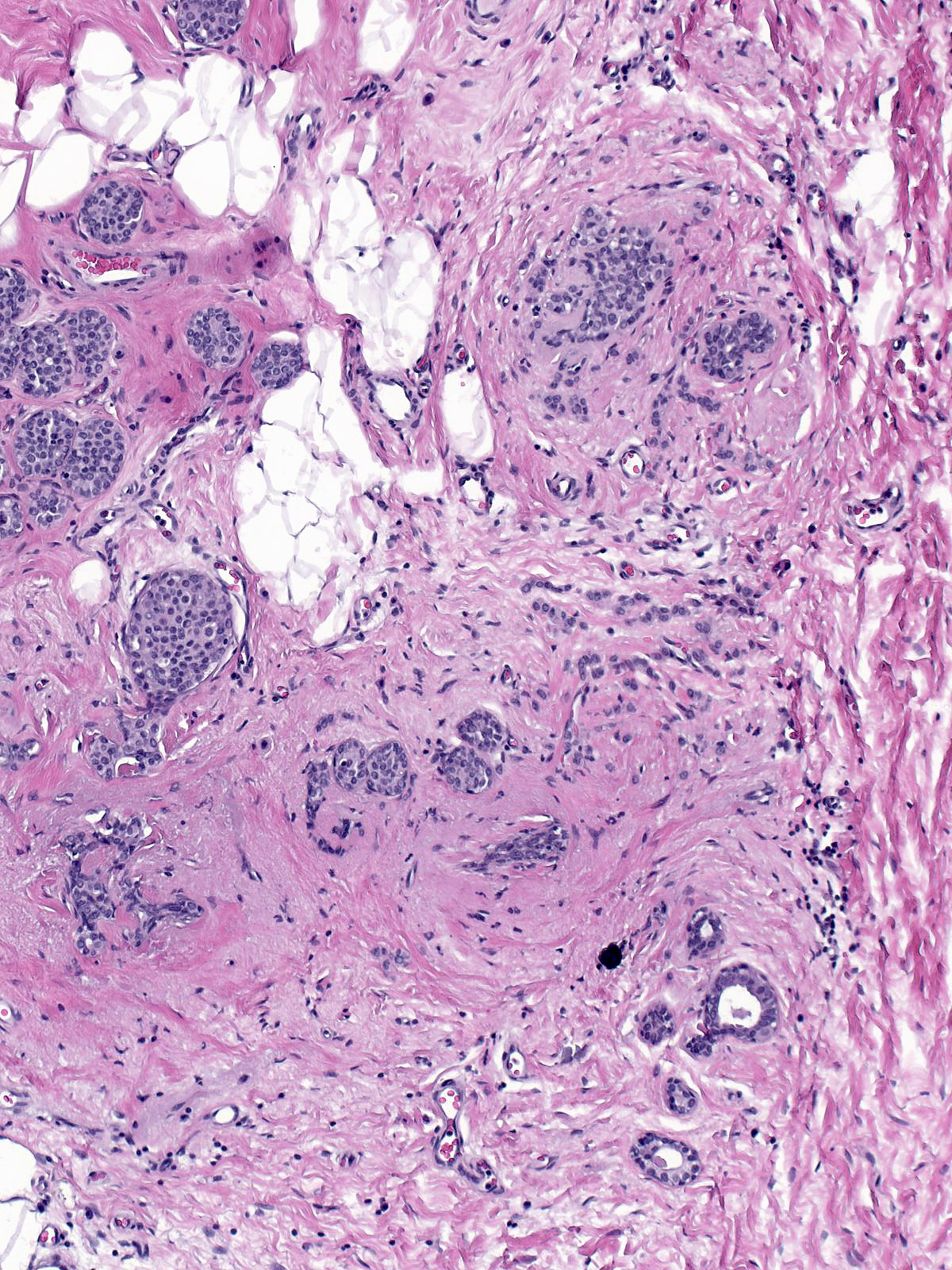
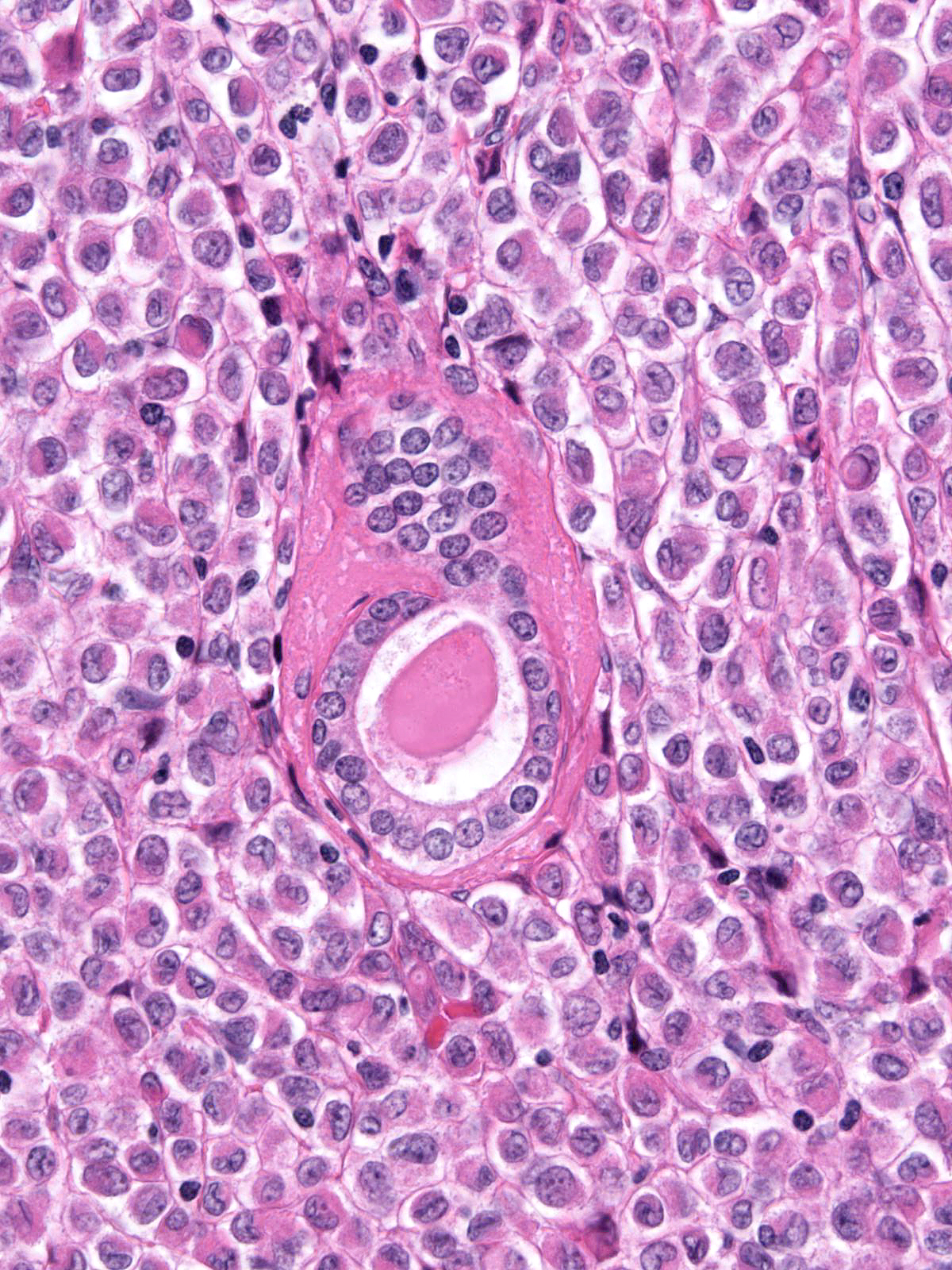
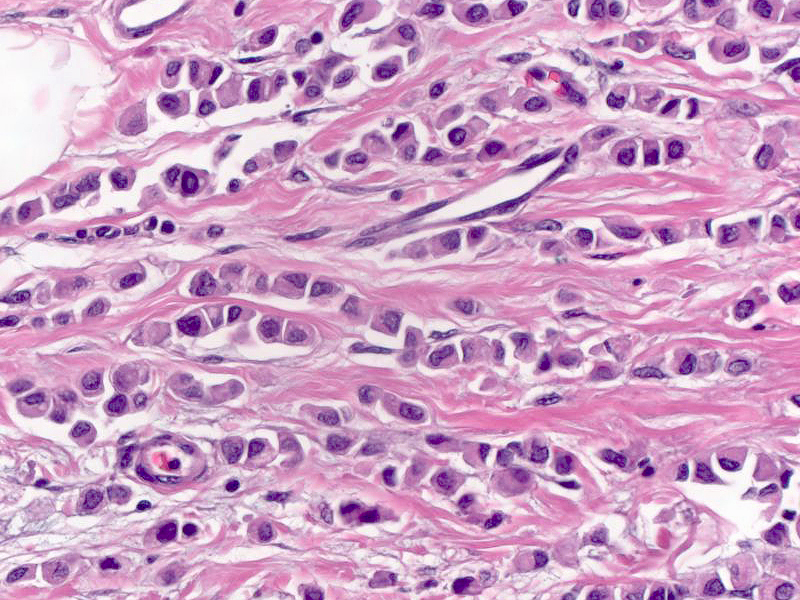
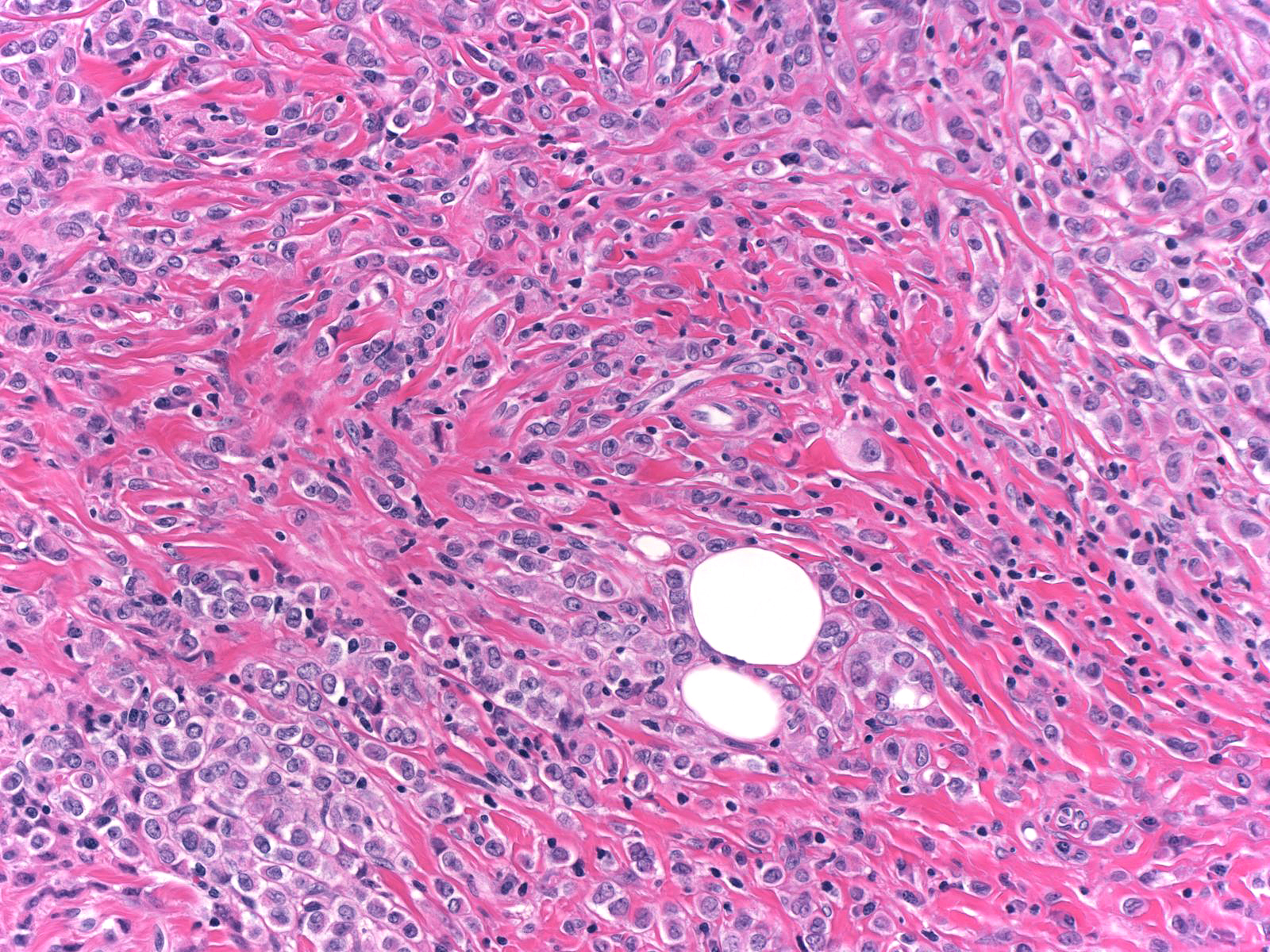
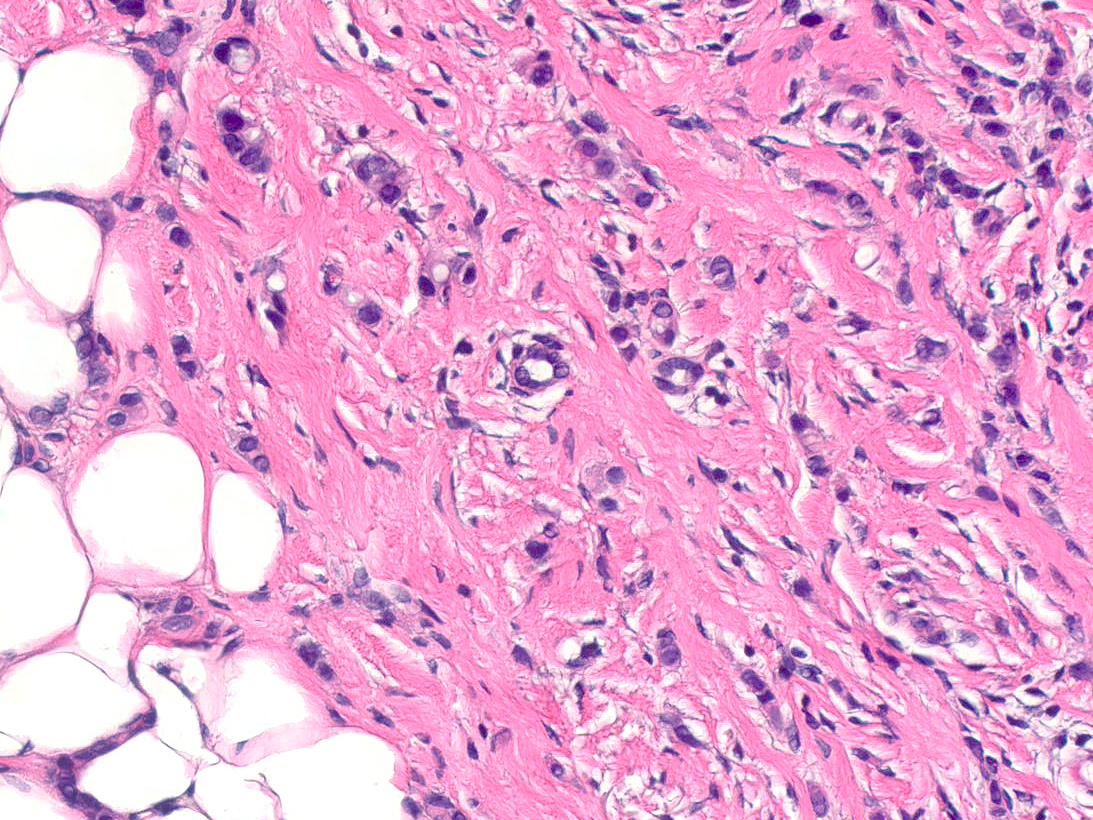
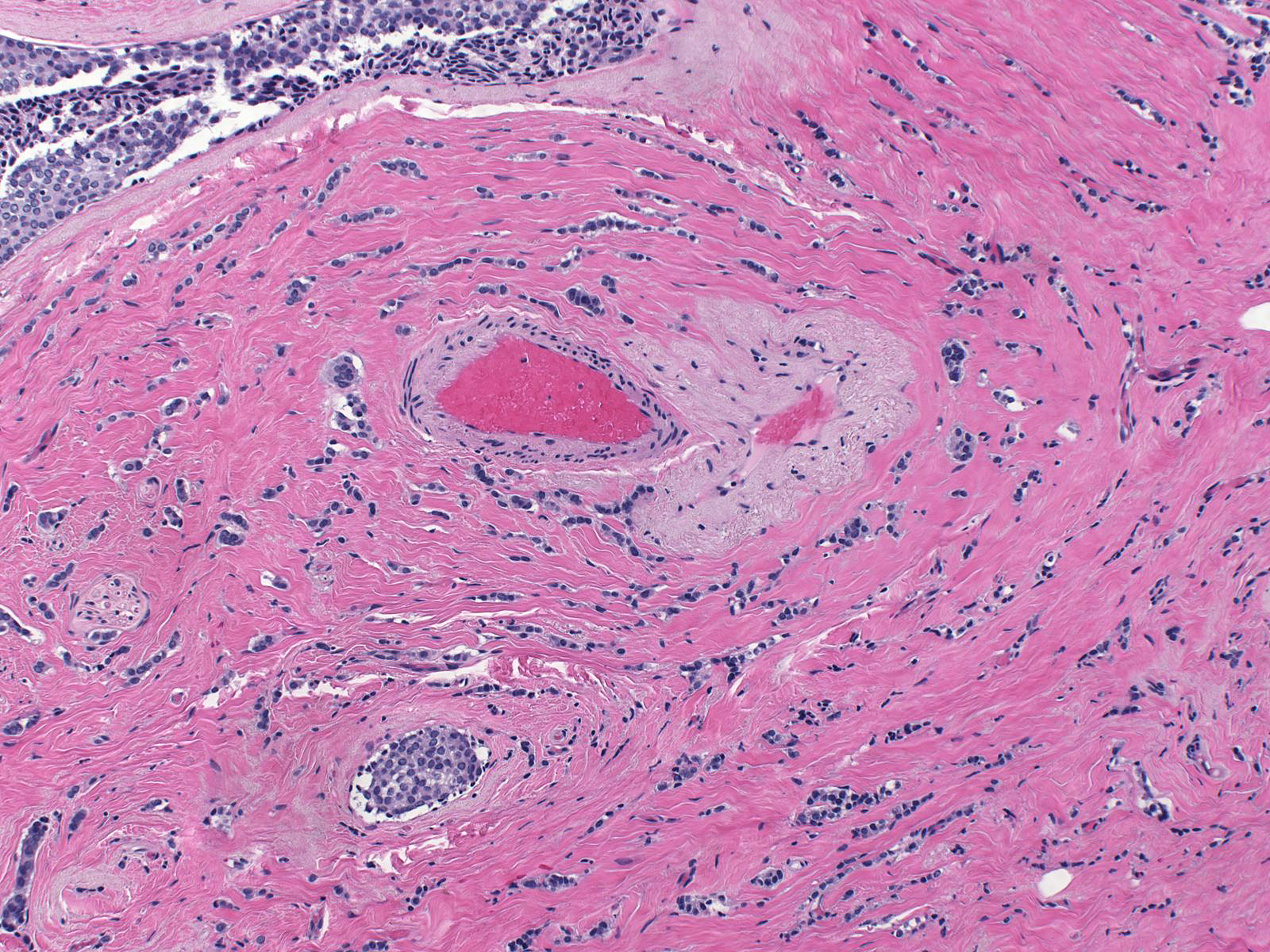
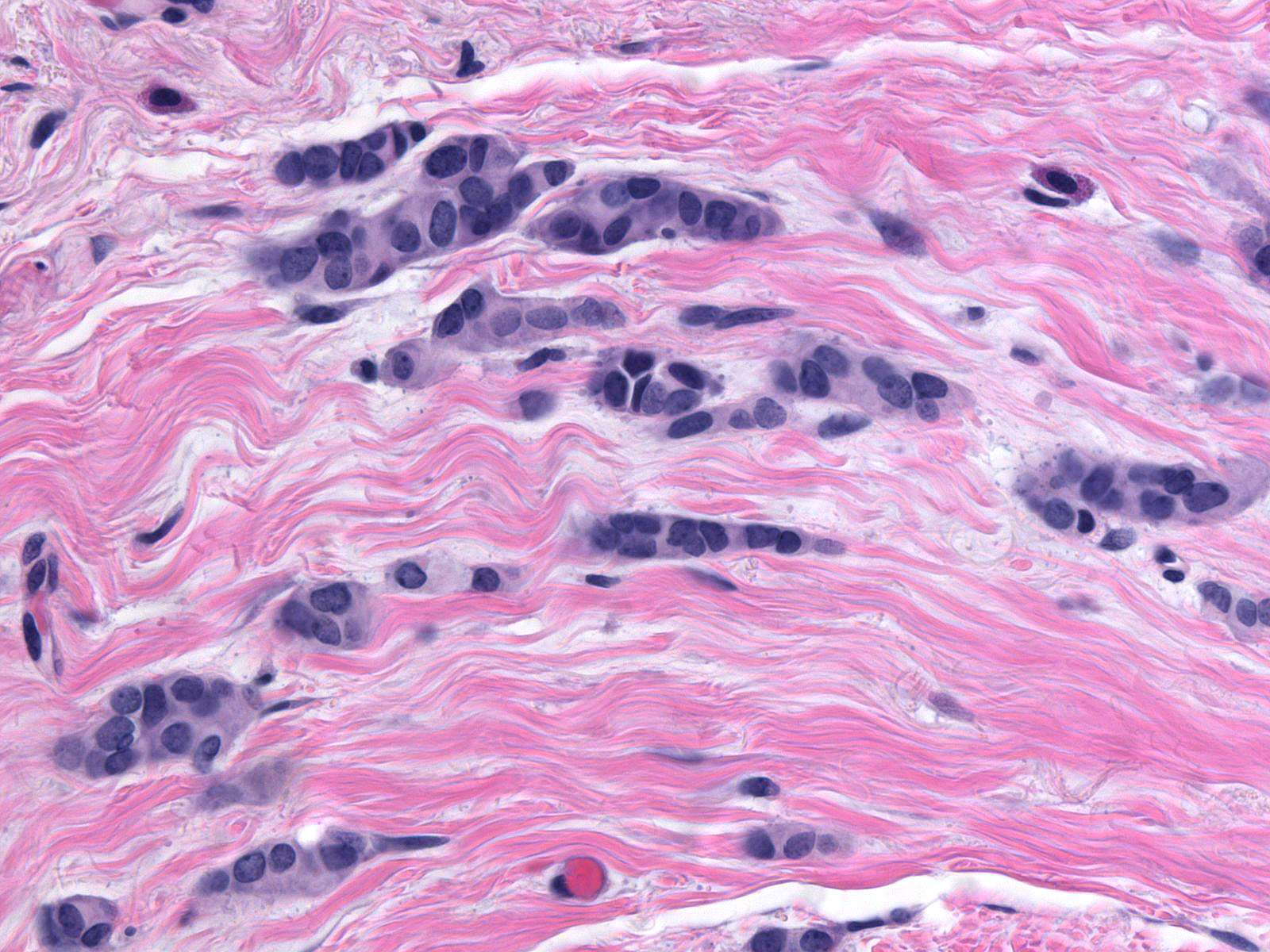
The invasive cells grow in single-file chains and loose columns (left), which sometimes swirl around pre-existing ductules, acini, and small blood vessels (right).
| Close apposition of the cells gives rise to a compact appearance, but careful inspection reveals that the cells do not adhere to each other even when closely packed. |
 |
|
|
| The stroma may display a slight desmoplastic reaction, but it often appears completely unaffected. |
 |
|
|
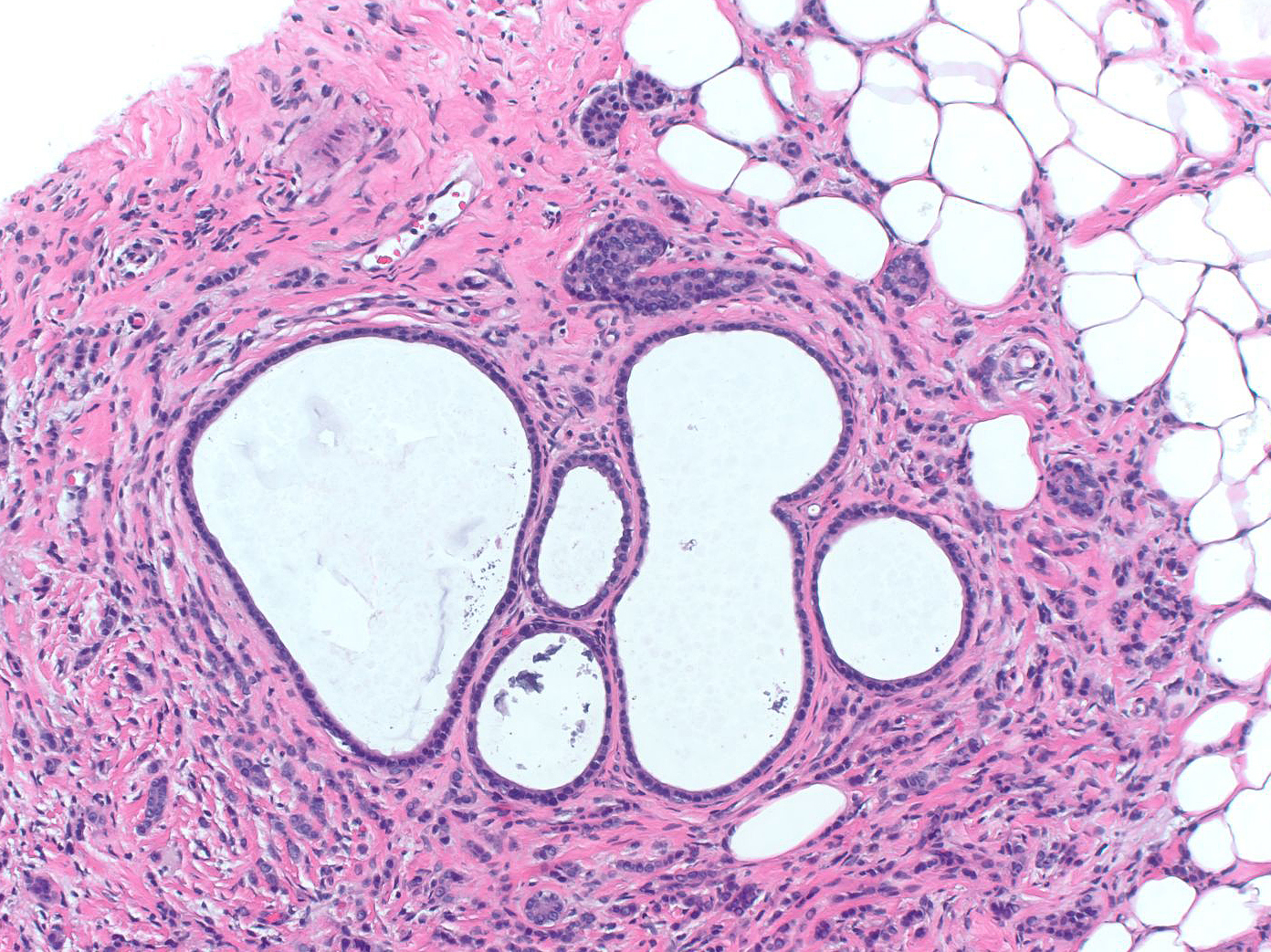
| Besides forming chains and narrow columns, the cells can form tubule-like structures. |
 |
|
|
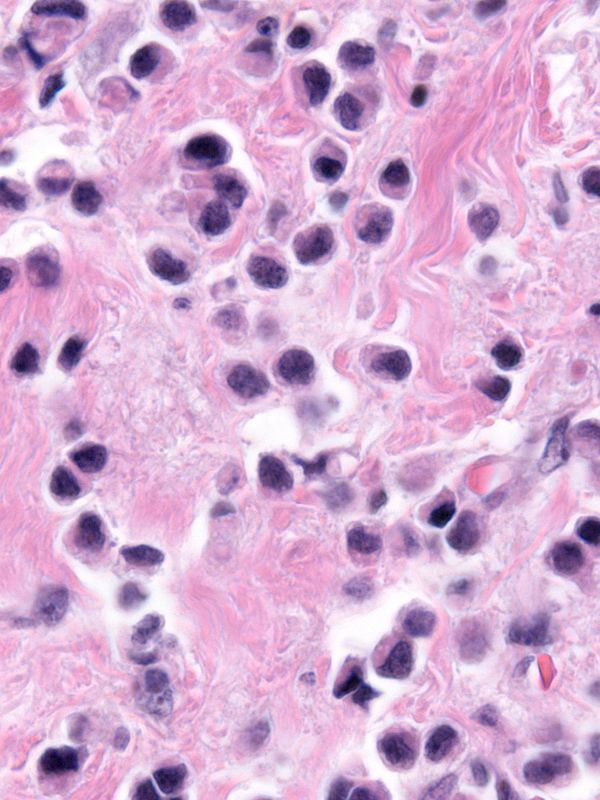
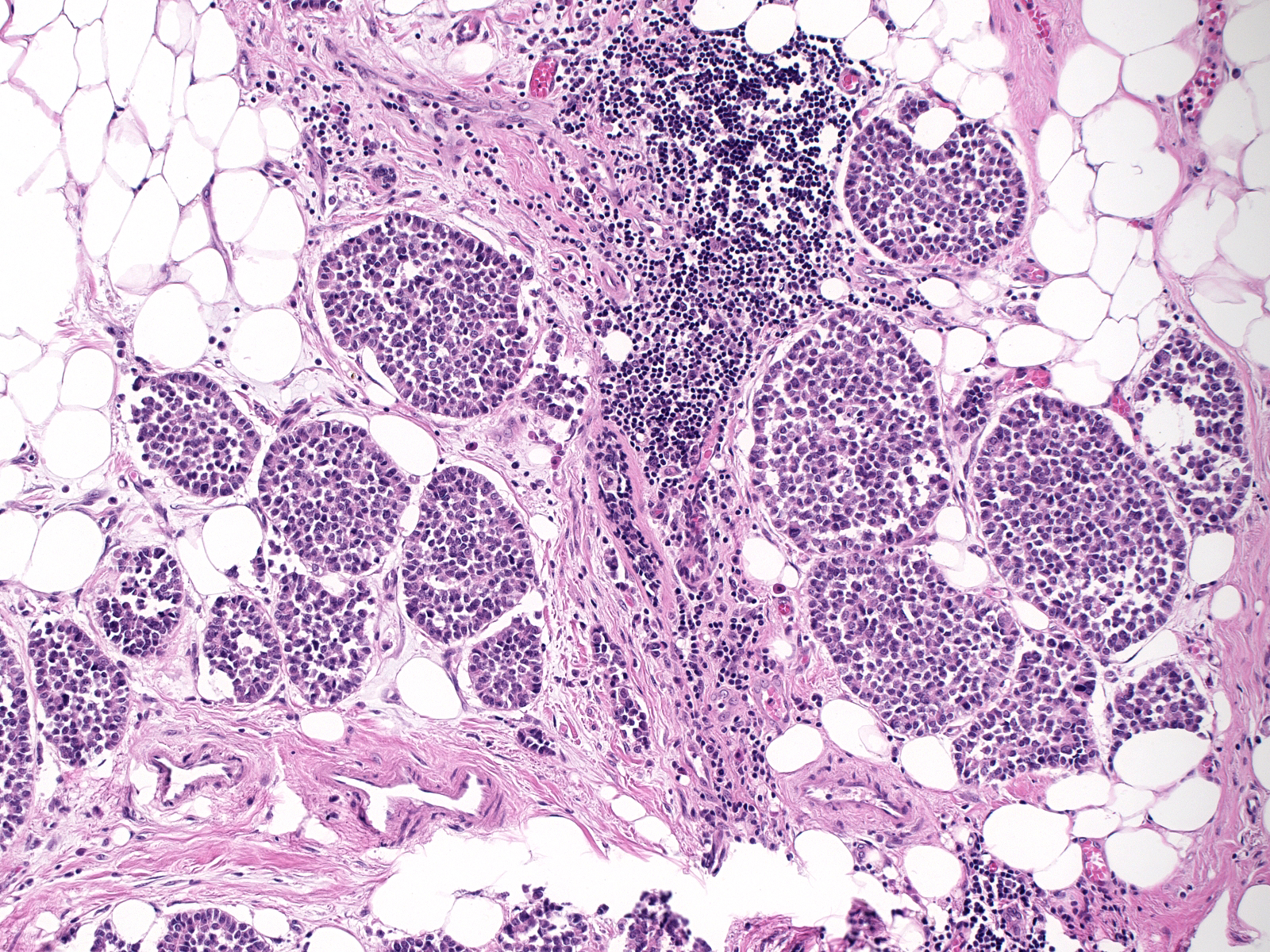
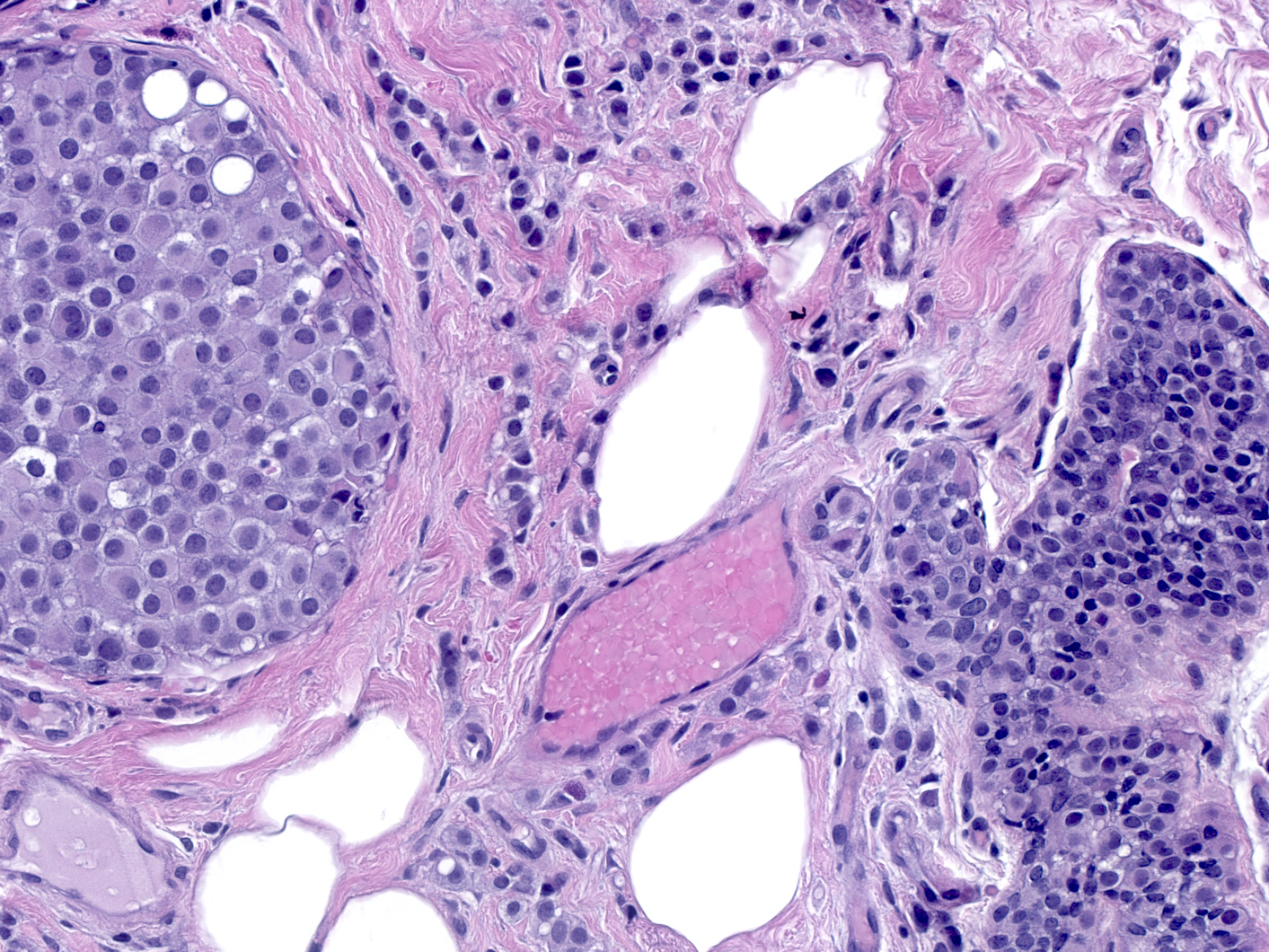
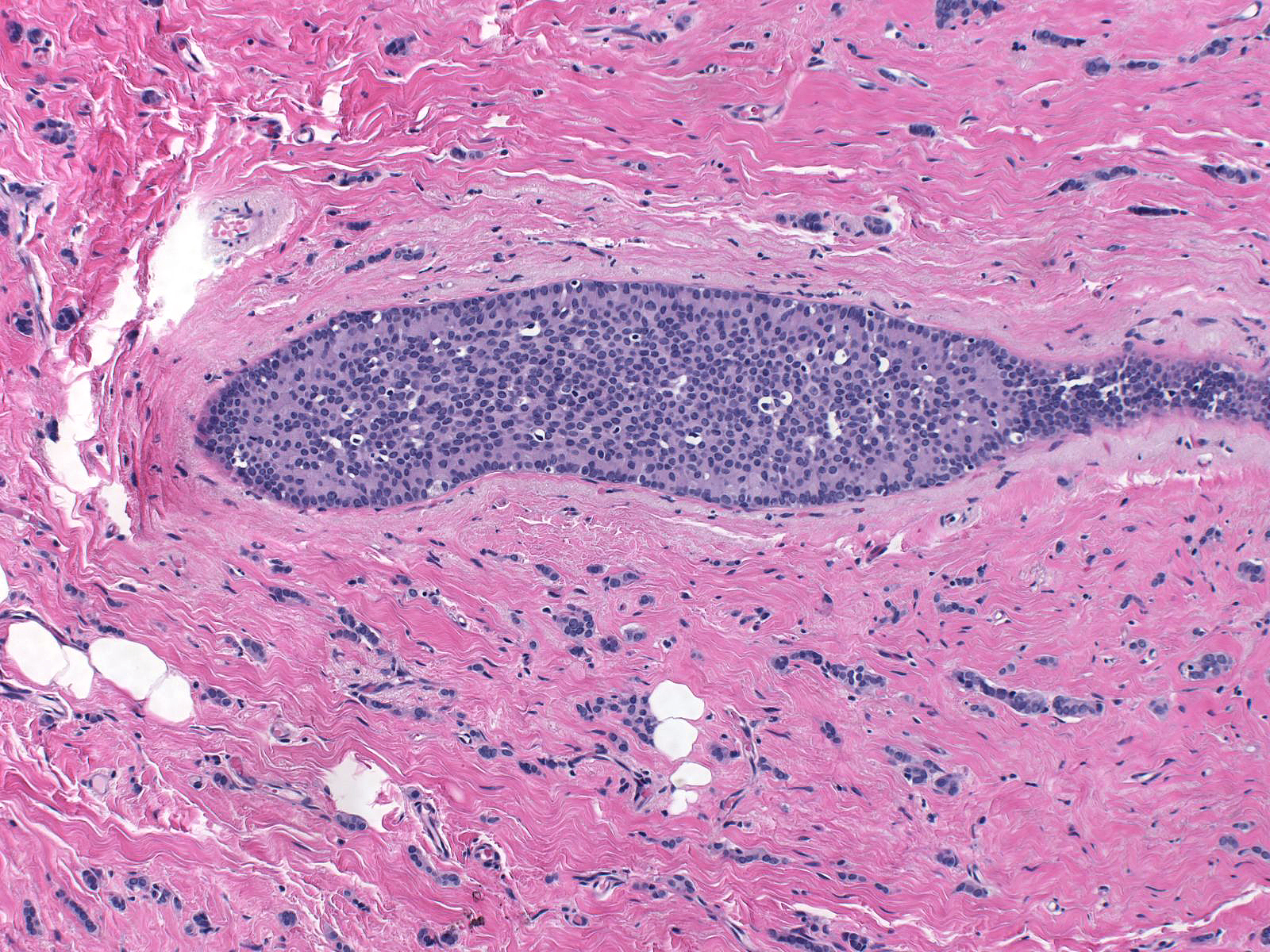
The cells can also accumulate in loose clusters. Pathologists refer to this as the alveolar pattern. One can easily mistake these alveolar nests as foci of lobular carcinoma in-situ.
| Close inspection of tubule-like structures and nests shows that the cells composing them do not possess significant amounts of apical cytoplasm or display clear-cut polarization and that the cells within the nests retain their dishesive properties. |
 |
|
|
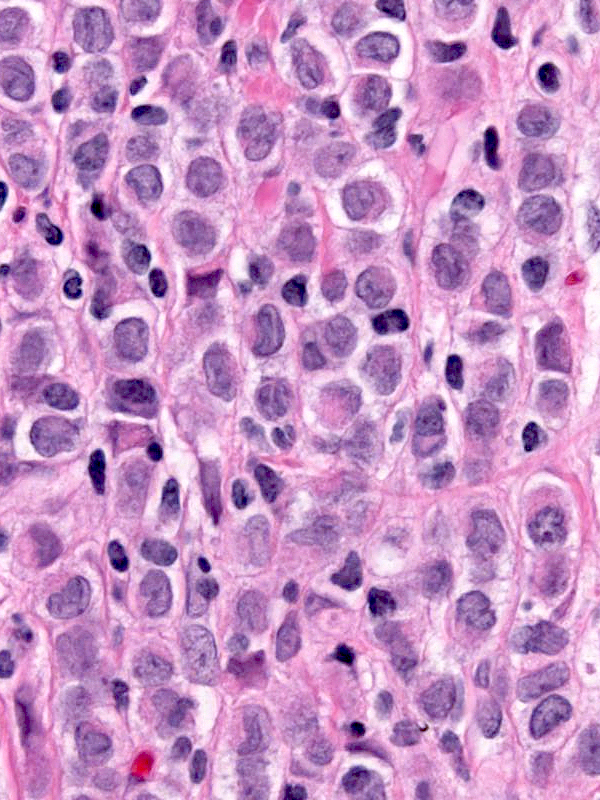
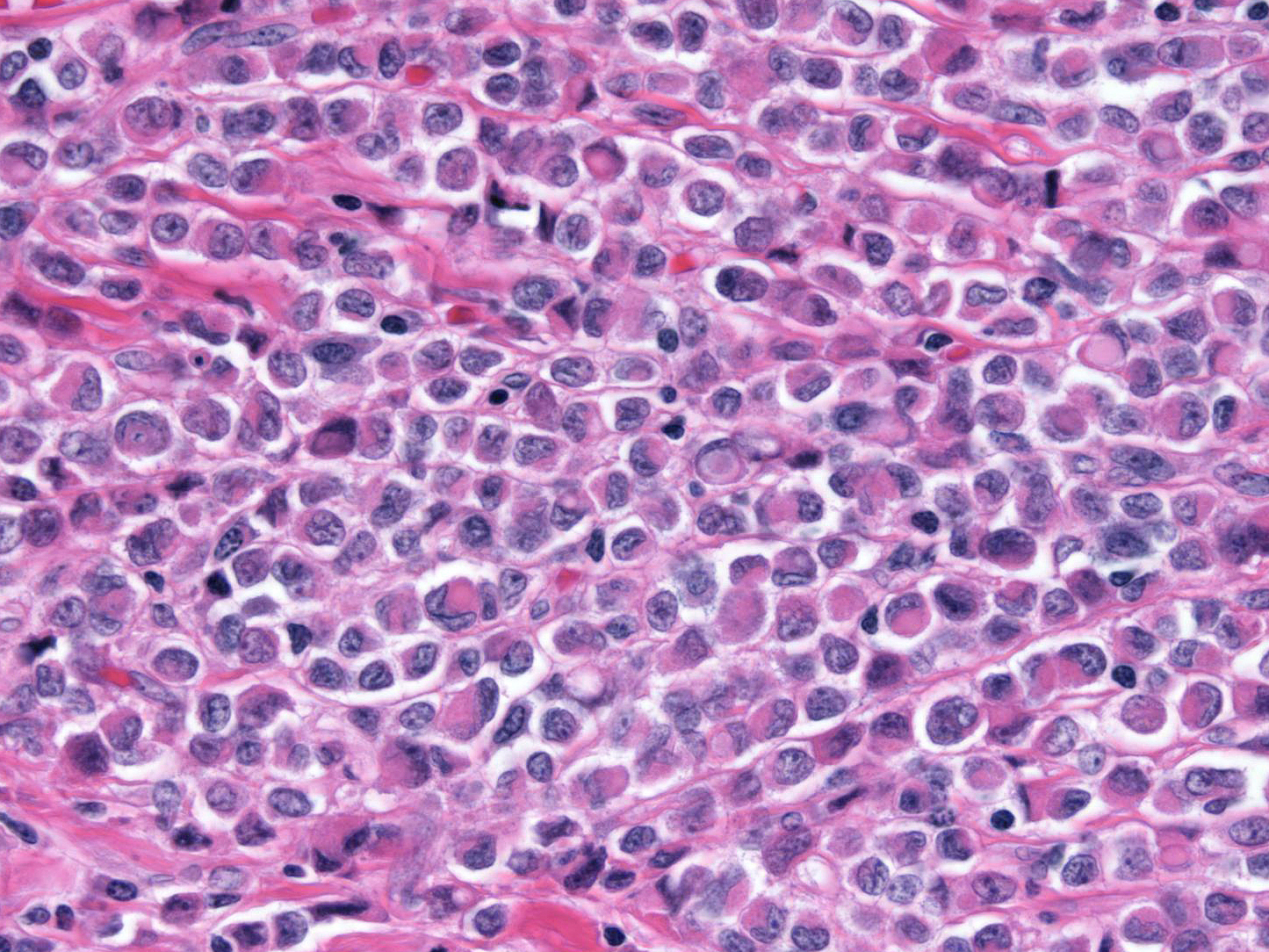
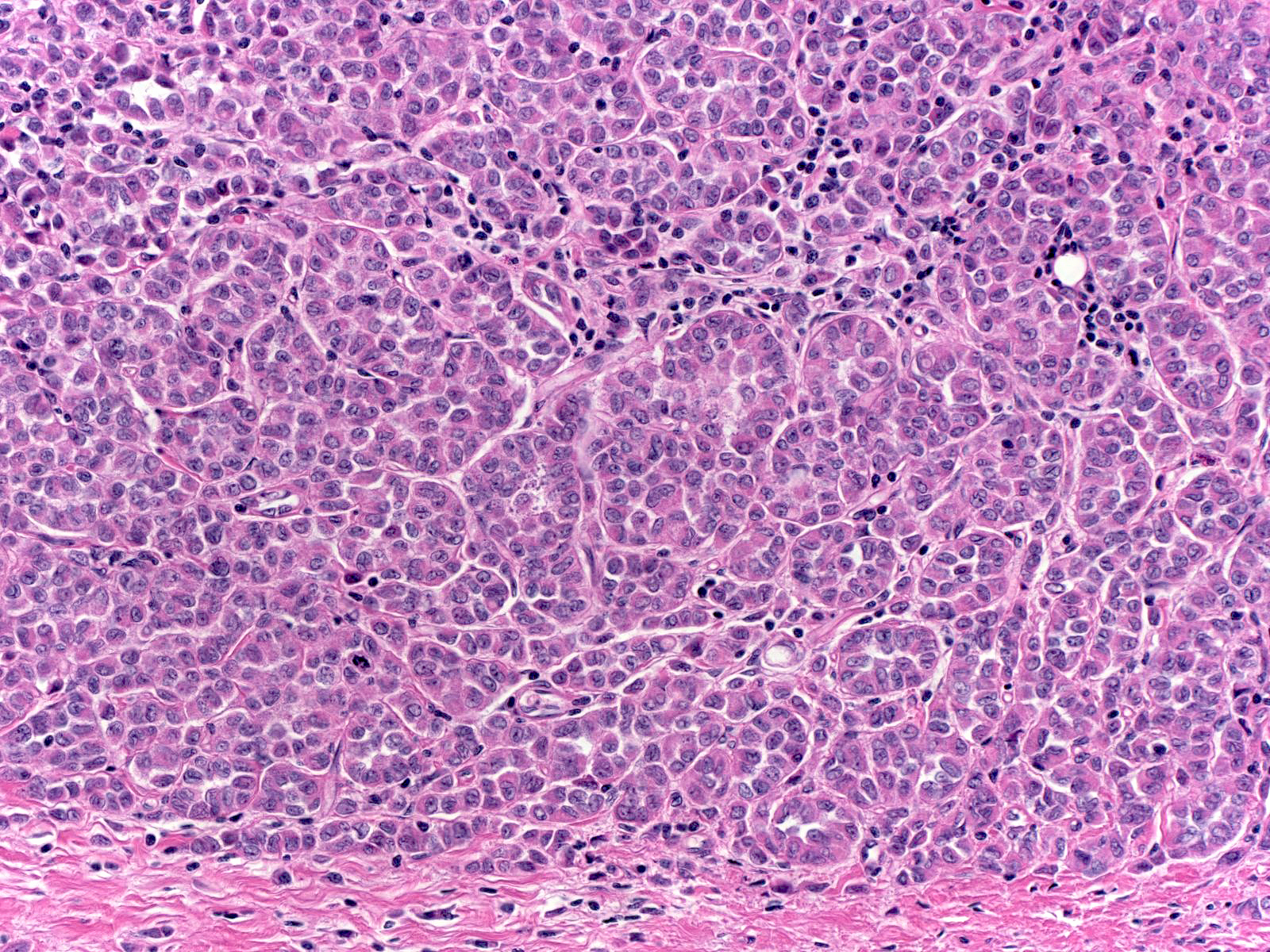
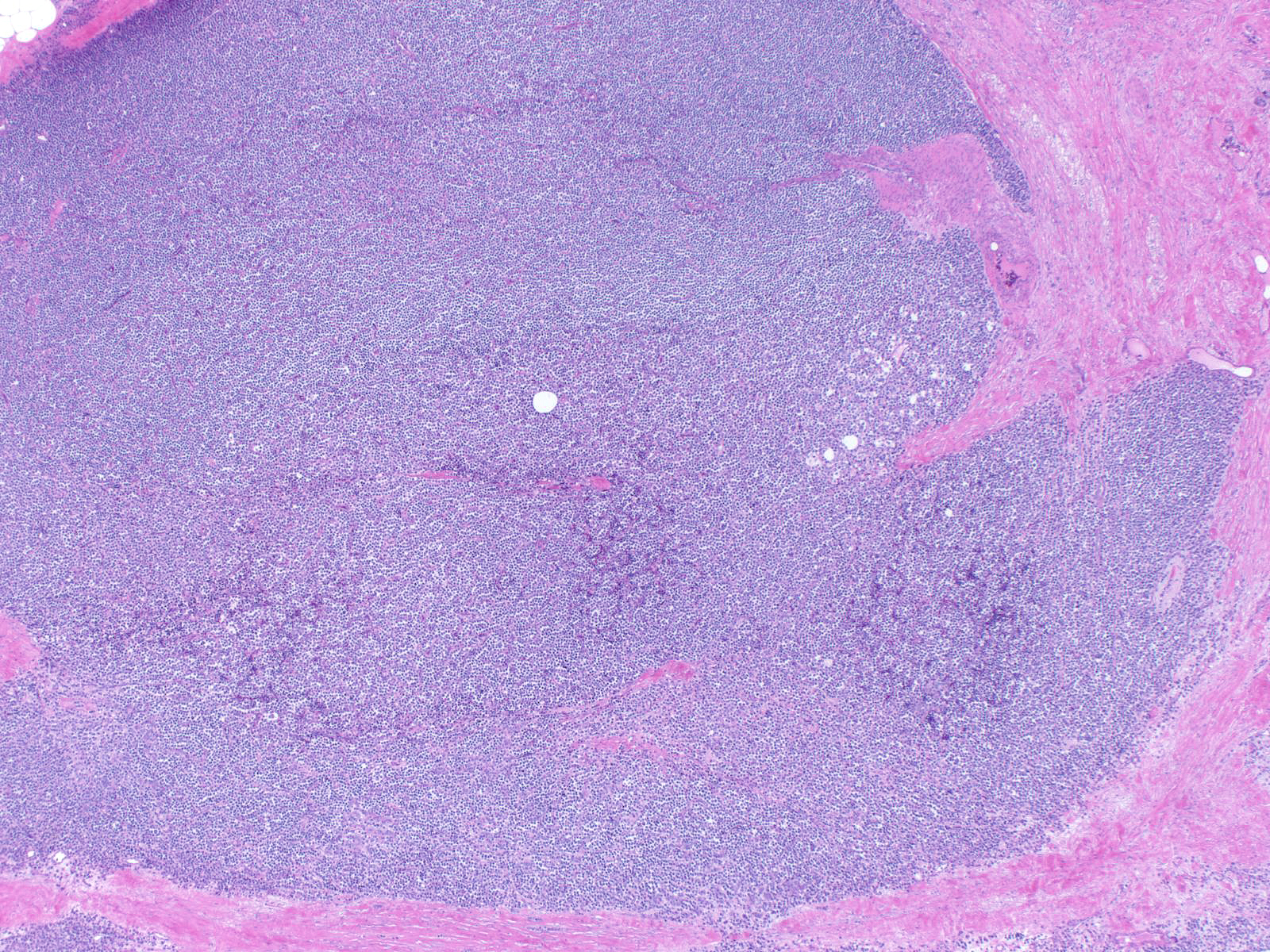
| When the carcinoma cells aggregate in a large mass, they give rise to the solid pattern. |
 |
|
|
| These alternative growth patterns usually co-exist with the typical linear stranding pattern. |
 |
|
|
Camouflaged ILC
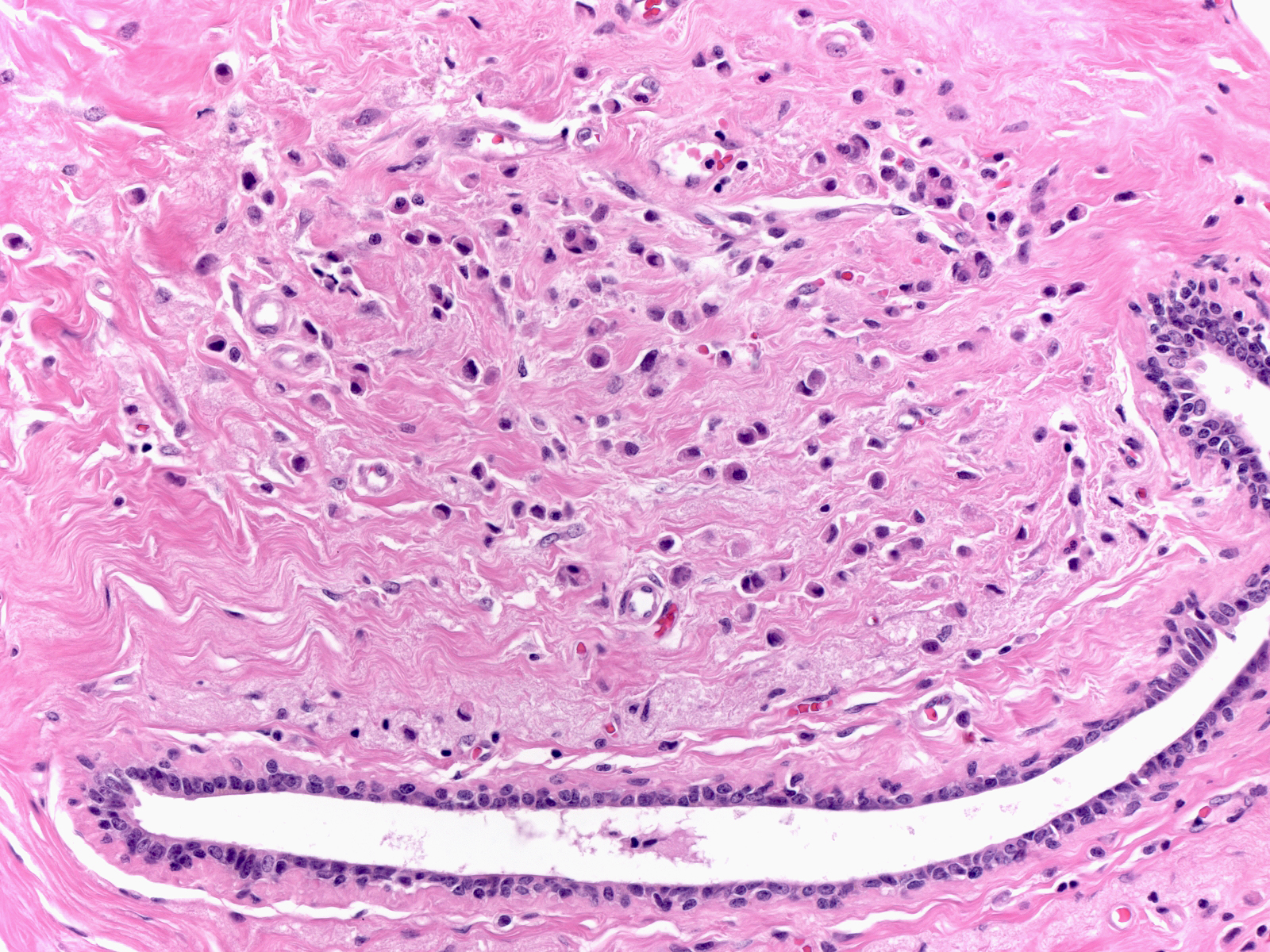
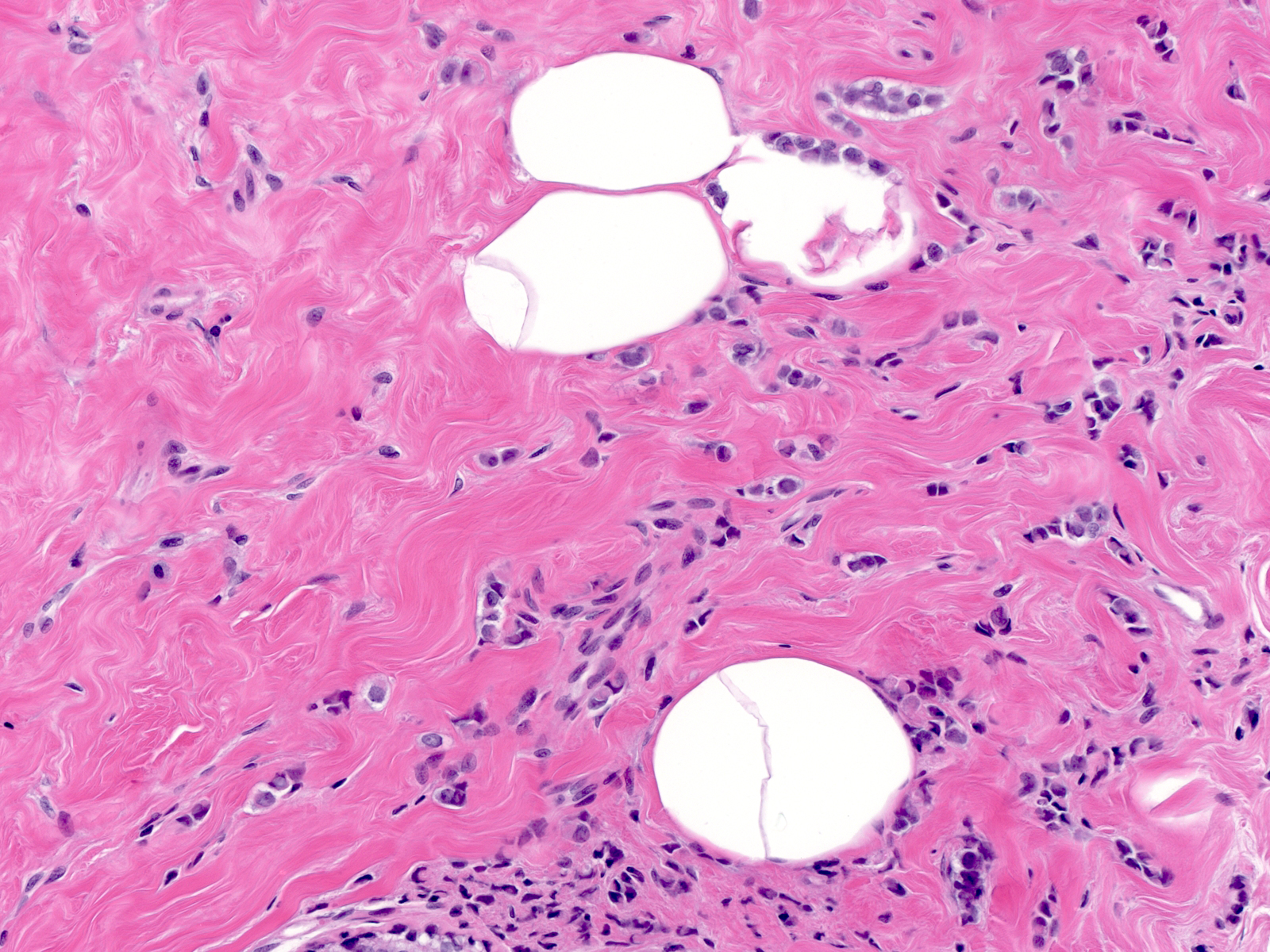
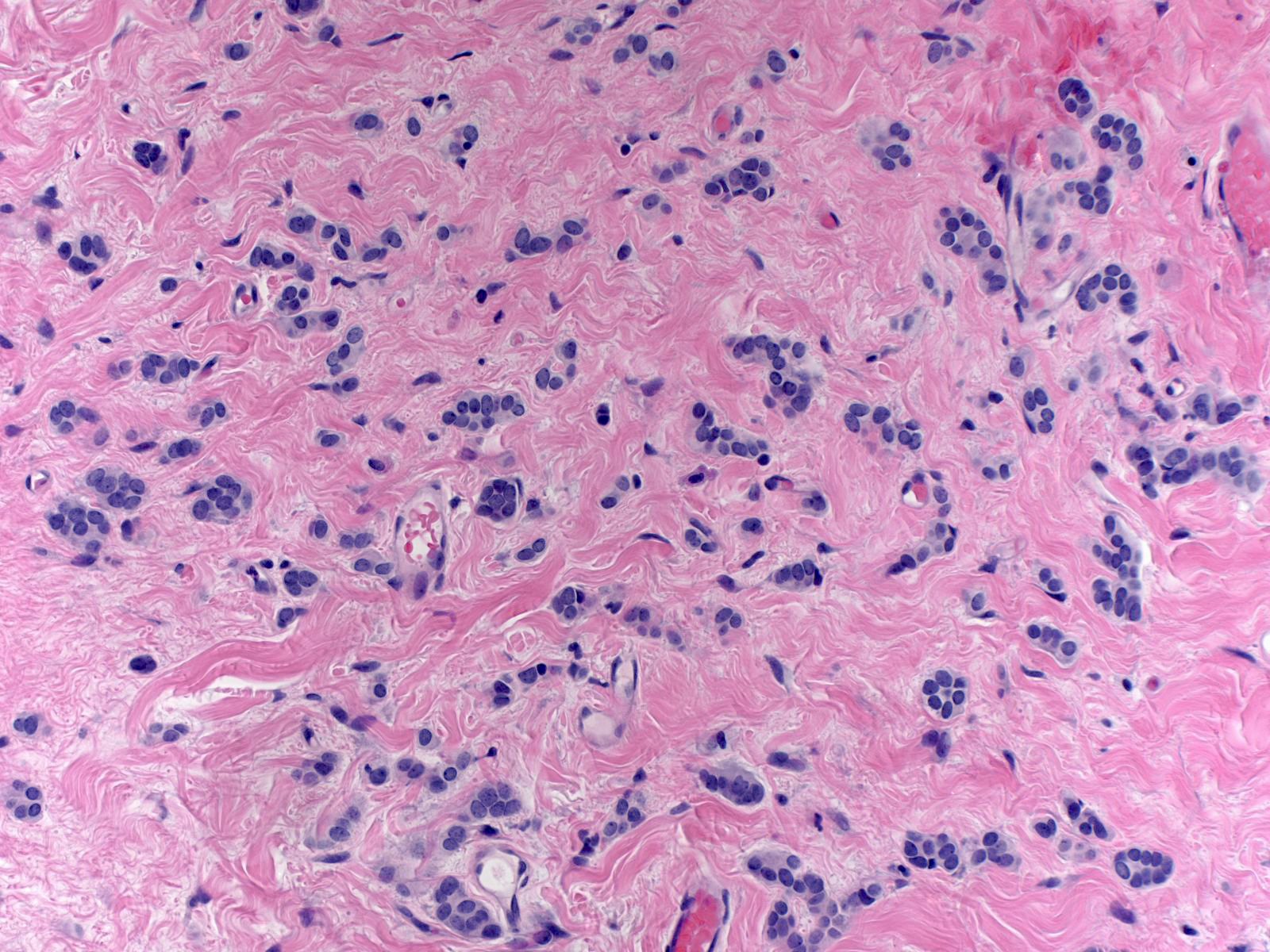
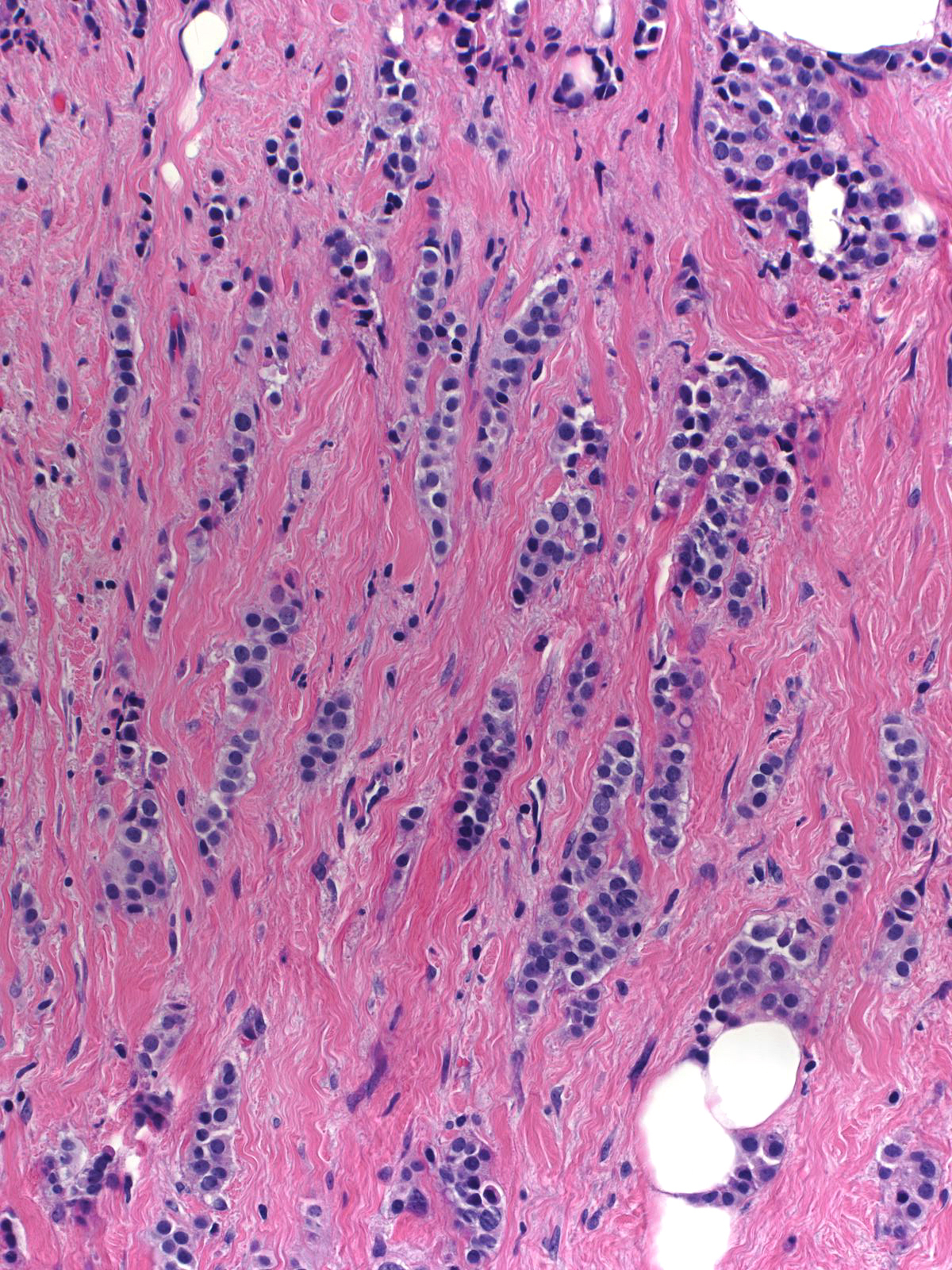
Small foci of invasive lobular carcinoma can escape detection because they closely resemble chronic inflammatory cells (left) or stromal cells (right).
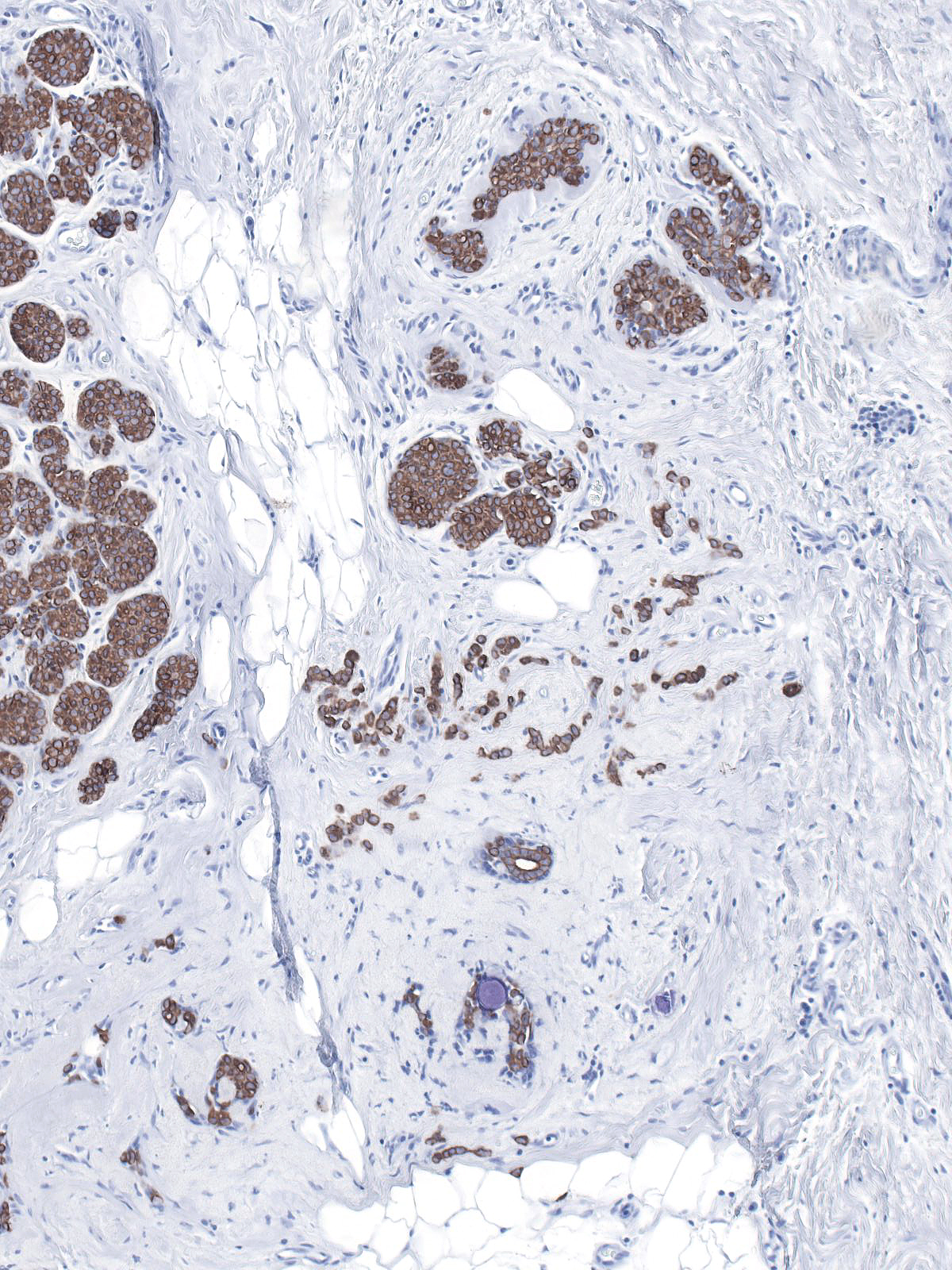
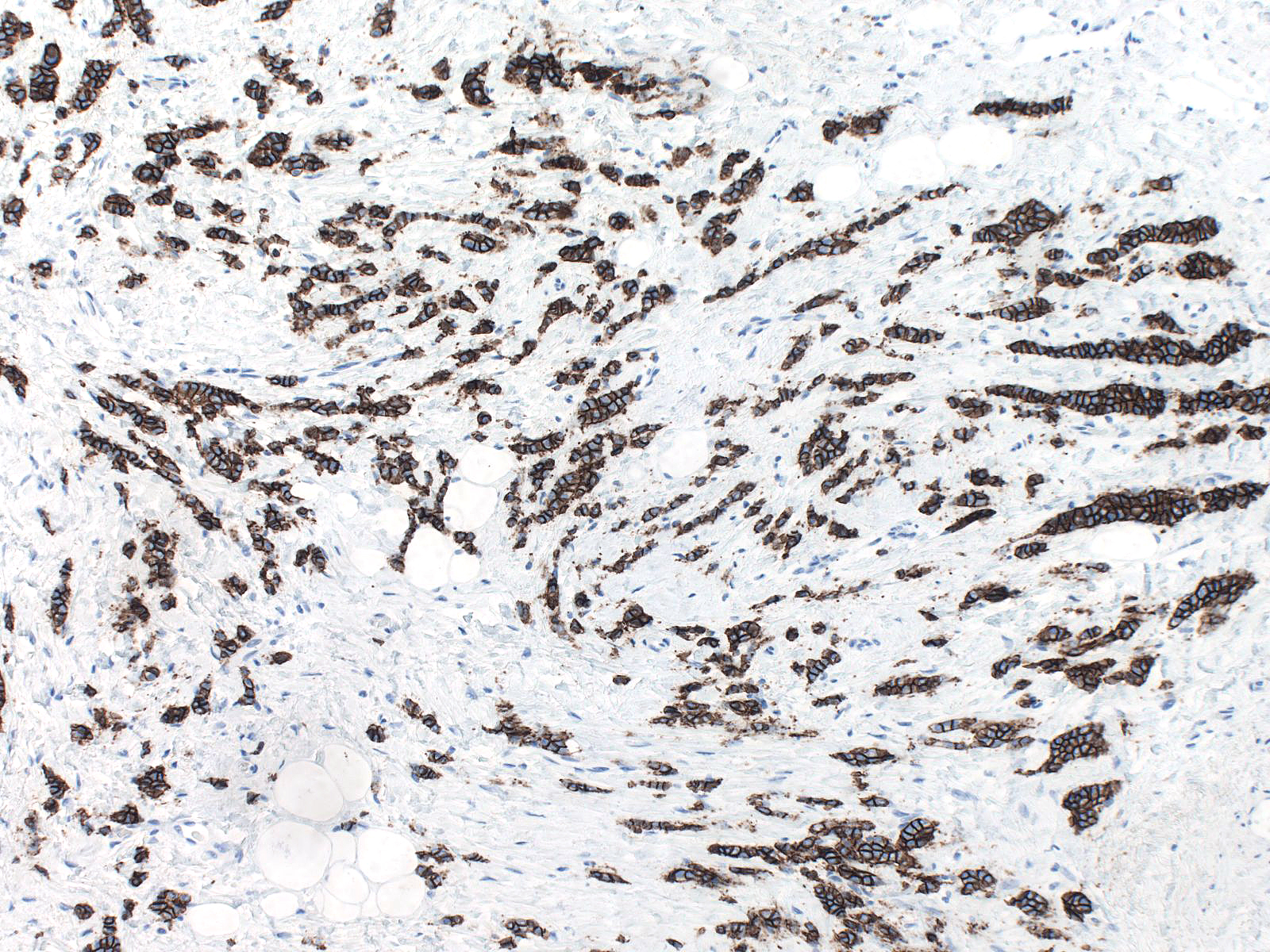
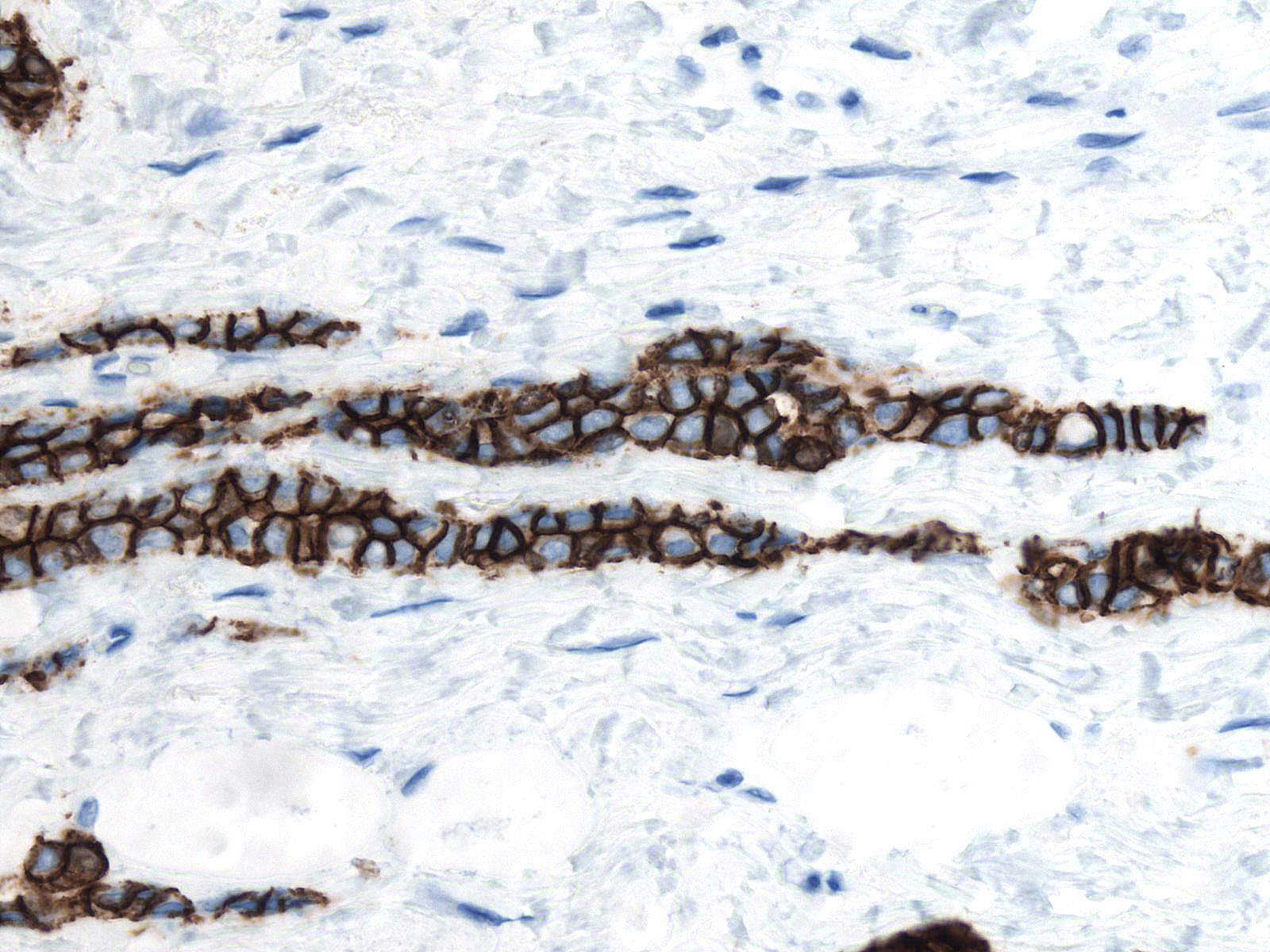
Staining for keratin can clarify the diagnosis in these difficult to detect foci!!!
Invasive Ductal Carcinoma Growing in a Dispersed Pattern
This invasive ductal carcinoma grows as small clusters and slender chains of cells in a pattern that brings to mind that of invasive lobular carcinoma (left); however, the in situ carcinoma grows in solid (center) and micropapillary (right) arrangements.
 |
 |
 |
| Invasive carcinoma growing in a dispersed fashion |
Solid DCIS |
Micropapillary DCIS |
Furthermore, the neoplastic cells form small clusters rather than growing as single cells (left). The close apposition of the cells in the clusters (center) and their molding around each other indicate a degree of intercellular cohesion. The carcinoma cells stain strongly for E-caherin (right).
 |
 |
 |
| Small agregates |
Cohesive clusters |
A stain for E-cadherin |
| Staining for E-cadherin demonstrates the pattern characteristic of ductal cells. |
 |
|
|
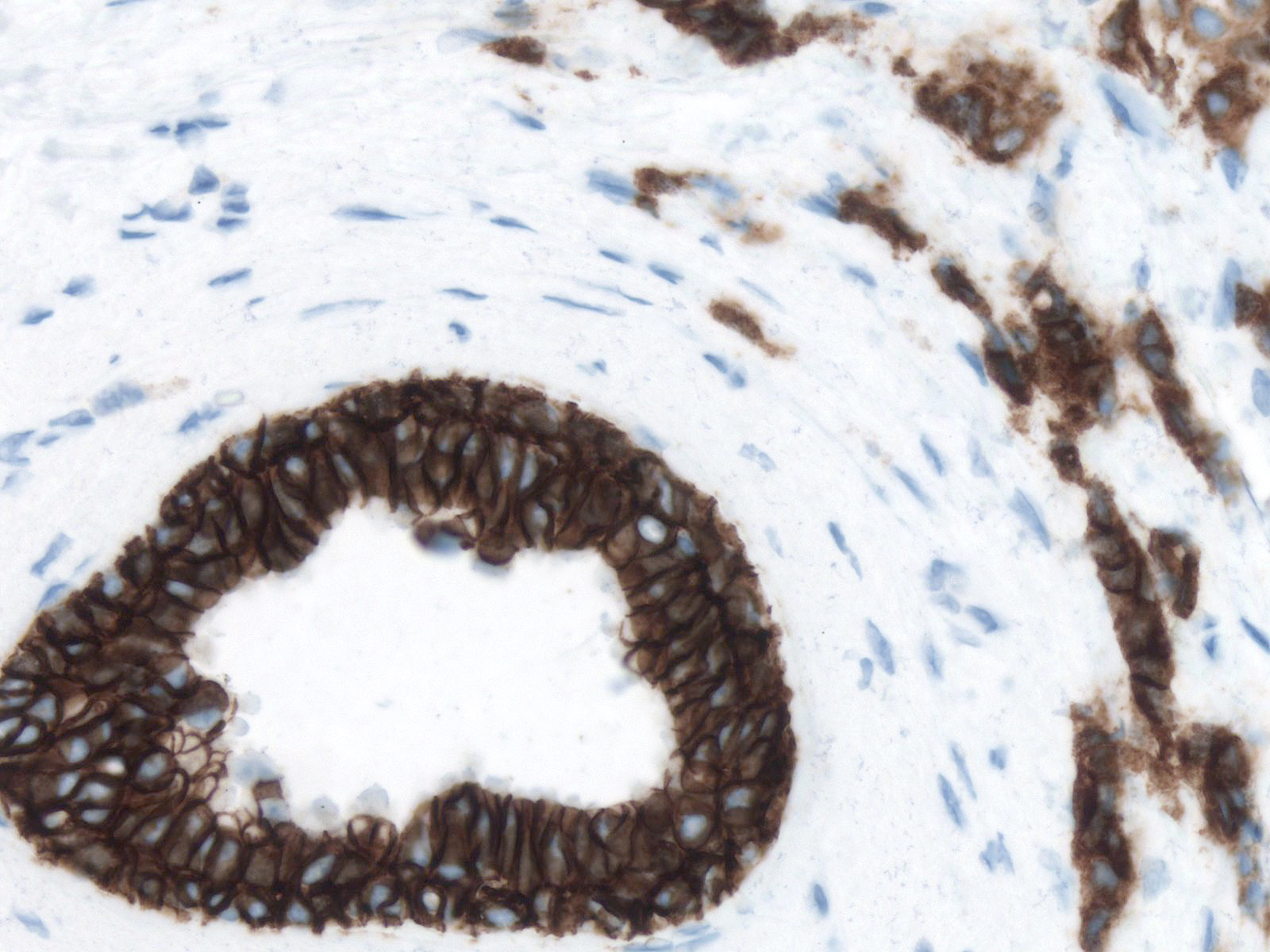
Note the strong linear staining limited to the lateral aspects of the cells evident in this stain for E-cadherin.
Invasive Ductal Carcinoma with Altered Junctional Complexes
The invasive component of this carcinoma resembles invasive lobular carcinoma in many respects; however, the cells that compose the noninvasive component appear more cohesive than conventional neoplastic lobular cells, and the invasive cells stain for E-cadherin strongly.
 |
 |
 |
| Invasive carcinoma |
In-situ carcinoma |
A stain for E-cadherin |
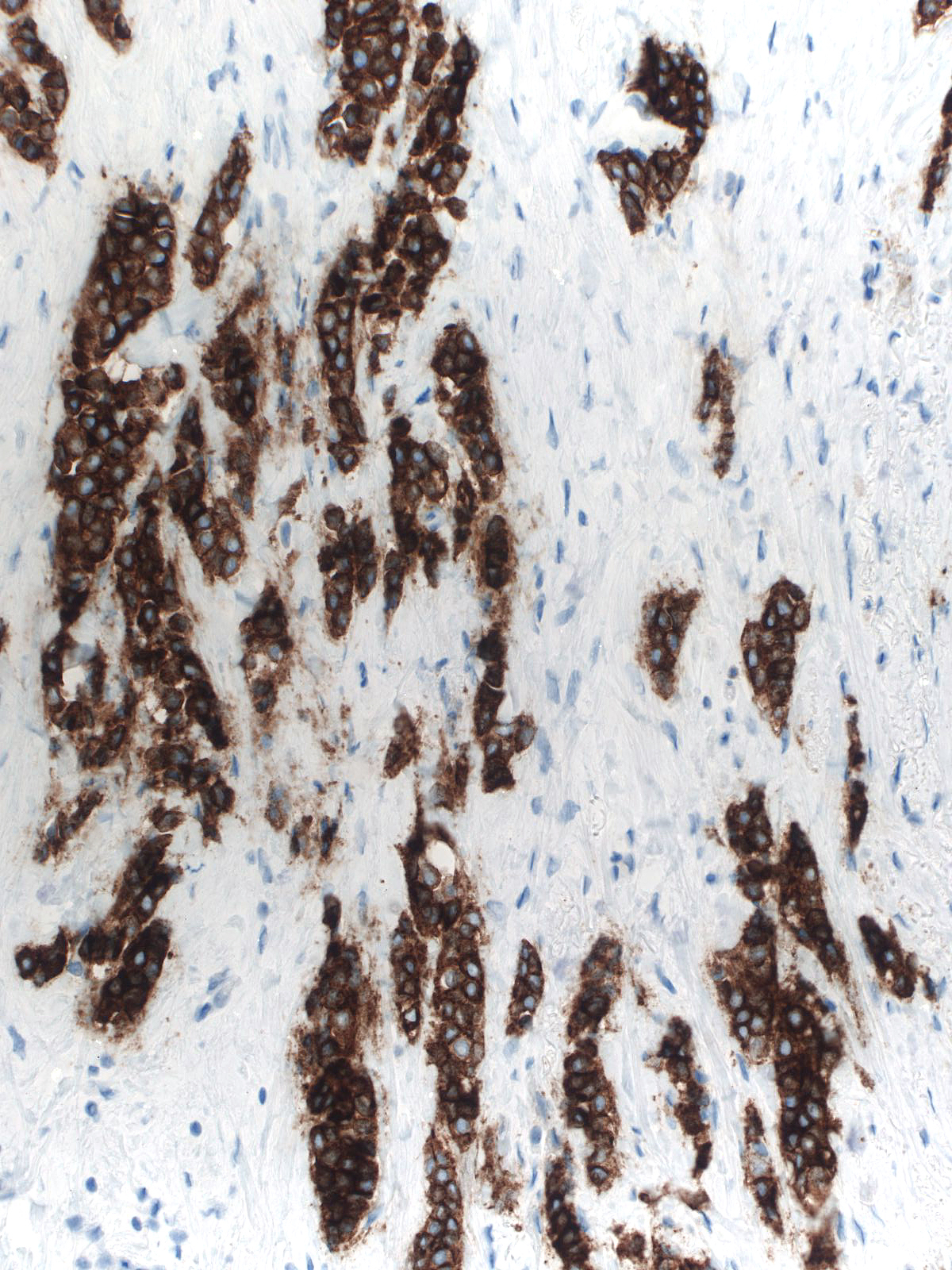
| Note that the cytoplasm of the tumor cells (upper right) rather than their cell membranes stains and that the staining appears diffuse and either granular or smudgy rather than linear and crisp as seen in normal luminal cells (bottom left). This localization of the E-cdherin in the cytoplasm indicates that the junctional complexes have not formed properly. One could surmise that the presence of defective complexes could give rise to many of the morphological features that develop because of the absence of E-cadherin and that carcinomas with altered complexes would therefore resemble typical lobular carcinomas. |
 |
|
|
A stain for E-cadherin
Breast Pathology