Difference between revisions of "Metaplastic Carcinoma"
(Created page with "__NOCACHE__{{DISPLAYTITLE:Metaplastic Carcinoma}} {{:TOC}} == General == Image:27-1 Osseous-CROP.jpg|thumb|The common subtypes of metaplastic carcinoma are spindle cell carc...") |
|||
| Line 41: | Line 41: | ||
{{img4|27-16 Chondroid.jpg|27-17 Osseous.jpg|Chondroid matrix|Osseous matrix}} | {{img4|27-16 Chondroid.jpg|27-17 Osseous.jpg|Chondroid matrix|Osseous matrix}} | ||
{{img1|When matrix-producing carcinomas form extensive matrix, they resemble chondrosarcomas or osteosarcomas.|27-18 Osteosarcoma.jpg}} | {{img1|When matrix-producing carcinomas form extensive matrix, they resemble chondrosarcomas or osteosarcomas.|27-18 Osteosarcoma.jpg}} | ||
| − | + | {{:mgh:breast-footer}} | |
| − | |||
| − | |||
Revision as of 19:15, July 13, 2020
General

- Definition: Metaplastic carcinoma represents a type of invasive ductal carcinoma. The histological characteristics of metaplastic carcinomas vary, but the presence of morphological attributes not characteristic of glandular cells stands as the defining attribute. Pathologists divide commonly encountered metaplastic carcinomas into two subtypes: spindle cell carcinoma and matrix-producing carcinoma. Extremely rare types of metaplastic carcinoma have regions with liposarcomatous, rhabdomyosarcomatous, angiosarcomatous, choriocarcinomatous, or melanocytic differentiation, among others.
- Clinical Significance: The clinical and radiological features do not differ from those of conventional invasive carcinomas. Metaplastic carcinomas tend to affect women in their seventh or eighth decade of life. They almost never occur in men.
- Gross Findings: Metaplastic carcinomas look like usual invasive ductal carcinomas.
- Microscopic Findings: The histologic characteristics depend on the subtype of metaplastic carcinoma.
- Differential Diagnosis: Fibromatosis (lack of carcinoma in‑situ and epithelial proteins, expression of ß‑catenin), phyllodes tumor with stromal overgrowth (presence of pre‑existing benign glands within the mass), sarcoma (Many types of sarcomas arise in the breast, but they do so only very, very rarely. Almost always, a spindle cell tumor will represent one of the other entities in the differential diagnosis rather than a sarcoma.)
- Discussion: To establish the diagnosis of metaplastic carcinoma, one must detect undisputable evidence of the epithelial nature of the malignant cells.
| The presence of associated ductal carcinoma in-situ and staining for epithelial proteins such as keratin and epithelial membrane antigen in many neoplastic cells would stand as secure evidence to establish the diagnosis of metaplastic carcinoma. |  |
Because metaplastic carcinomas vary in the type of keratin synthesized, one must use a panel of keratin stains to detect the presence of the protein. The panel should include several antibodies and cocktails of antibodies that react with keratin. Among anti‑keratin antibodies, CK903 (cytokeratin 34ßE12) and MNF116 offer the greatest sensitivity.
Spindle Cell Carcinoma
Pathologists subdivide the category of spindle cell carcinomas into two subgroups: low-grade (fibromatosis-like), and high-grade (sarcoma-like). Fibromatosis-like spindle cell carcinomas consist of spindle cells arranged in haphazardly disposed, short, interlacing fascicles. The cells contain scant cytoplasm and bland, spindly nuclei. Most tumors also contain small collections of epithelioid cells that possess dense eosinophilic cytoplasm. The malignant cells do not demonstrate nuclear pleomorphism or mitotic figures. The degree of collagen deposition varies from scant to abundant.
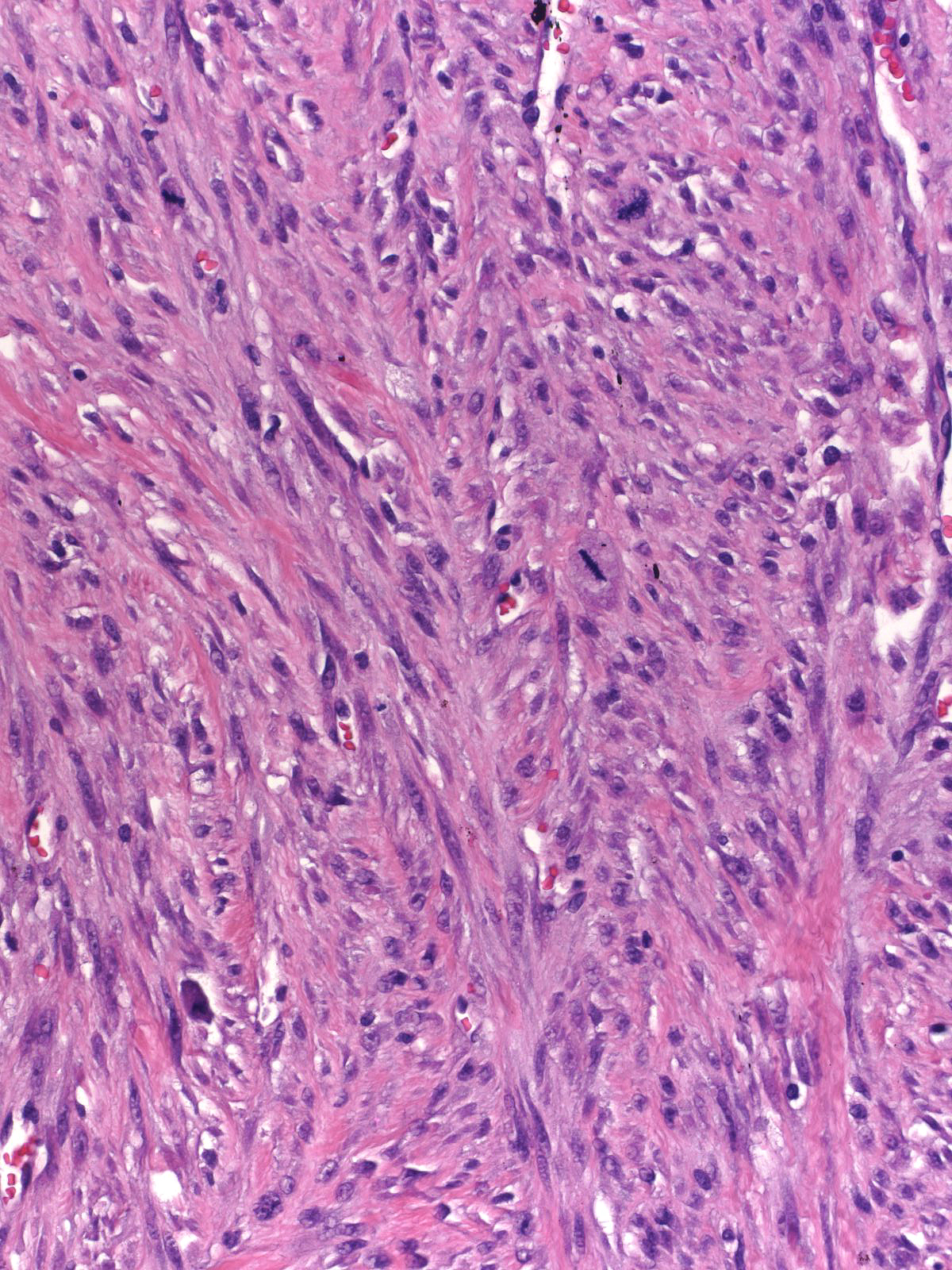
High-grade spindle cell carcinomas resemble high-grade fibrosarcomas.
High-grade spindle cell carcinomas consist of solid masses of spindly malignant cells with anaplastic nuclei and frequent mitotic figures.
 |
 |
One usually finds a few interspersed, clustered, epithelioid cells, which have oval to polygonal shapes and eosinophilic cytoplasm. These groups often display poorly developed squamous features, and these squamoid cells typically stain for cytokeratin.
 |
 |
| Besides growing in solid sheets and fascicles, the carcinoma cells can form branching strands. | 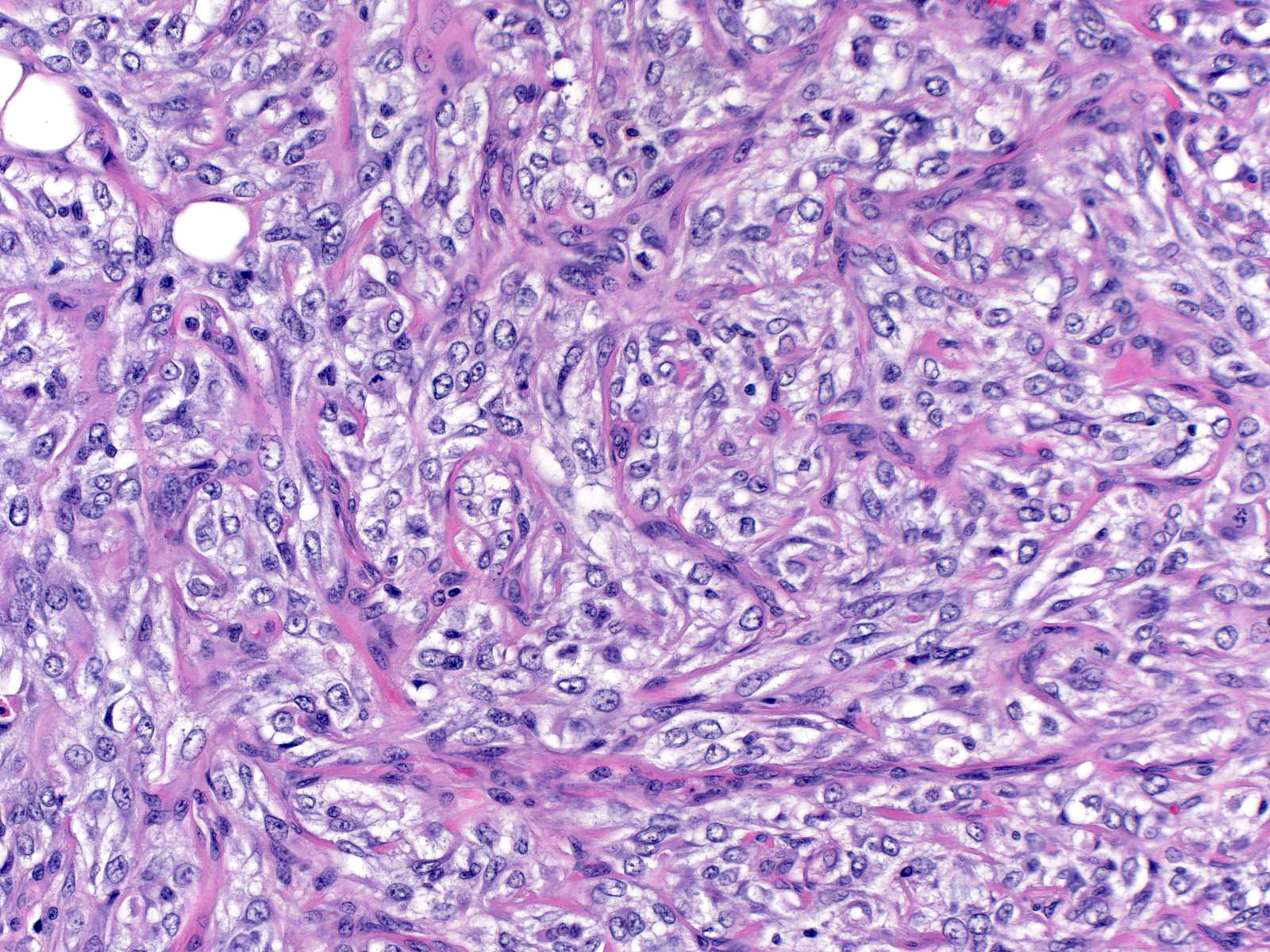 |
Loosening of the intercellular attachments within these strands gives rise to an appearance referred to as acantholytic or pseudovascular. Note the genuine blood vessel at the left edge of the left image. The pseudovascular spaces in the right image contain many eosinophils.
 |
 |
| The cells can produce abundant collagen. | 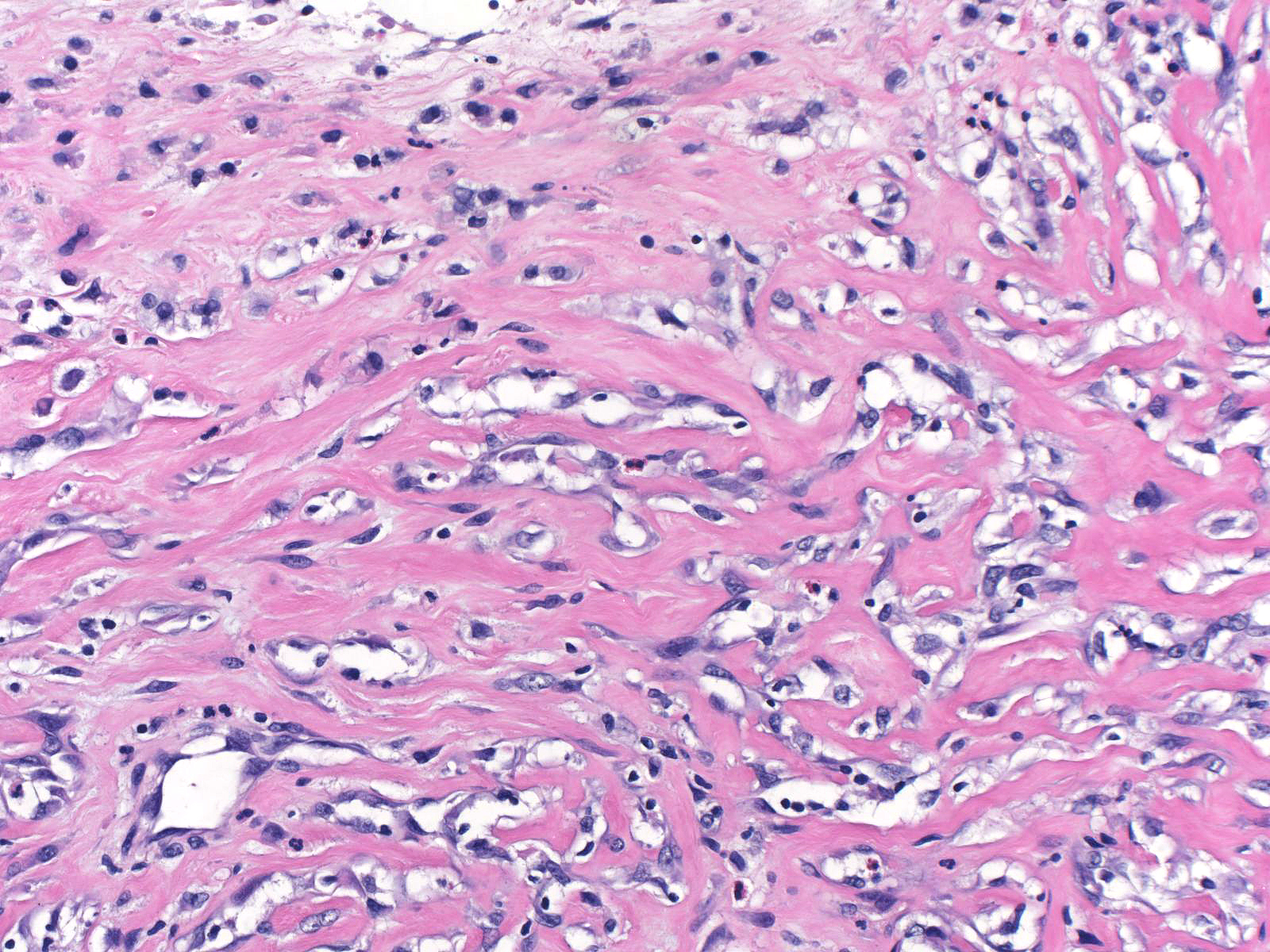 |
| Much less commonly, the neoplastic cells form glands. | 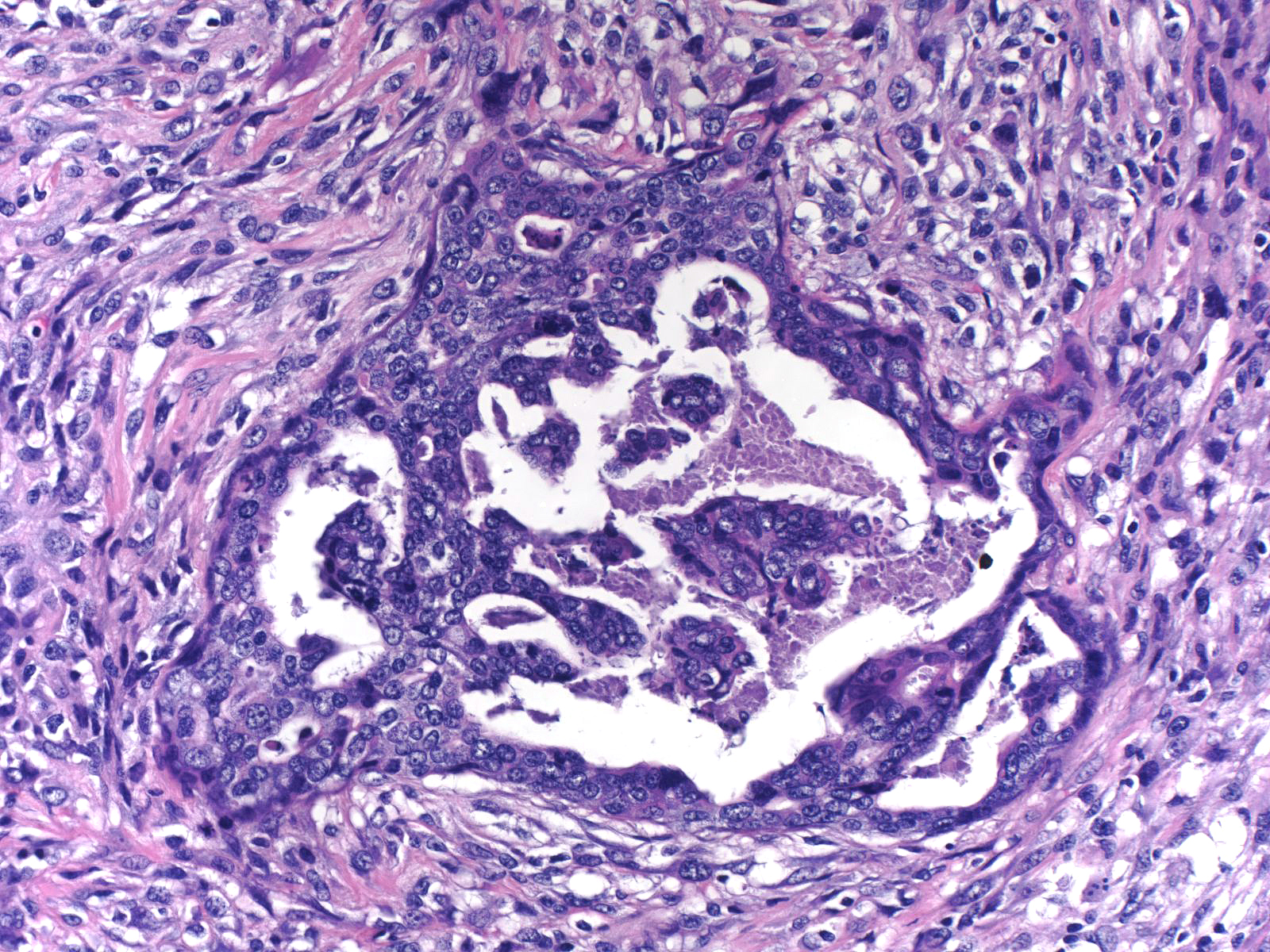 |
In addition to expressing keratin, many spindle cell carcinomas express p63.
 |
 |
Rare phyllodes tumors exhibit such extensive overgrowth of the stromal cells that the lesion comes to resemble a spindle cell tumor. The evaluation of two features helps to differentiate spindle cell carcinoma from phyllodes tumor with stromal overgrowth: the presence of benign glands within the mass, and the presence of ductal carcinoma in-situ. If the mass contains a component of benign glandular tissue, it is likely to be a phyllodes tumor. If the mass or adjacent tissue harbors ductal carcinoma in-situ, the mass is likely to be a spindle cell carcinoma. Extensive and robust staining of the spindle cells for keratin would also favor the diagnosis of spindle cell carcinoma; however, one must proceed cautiously, for the stromal cells in phyllodes tumors can produce modest amounts of keratin.
Matrix-producing Carcinoma
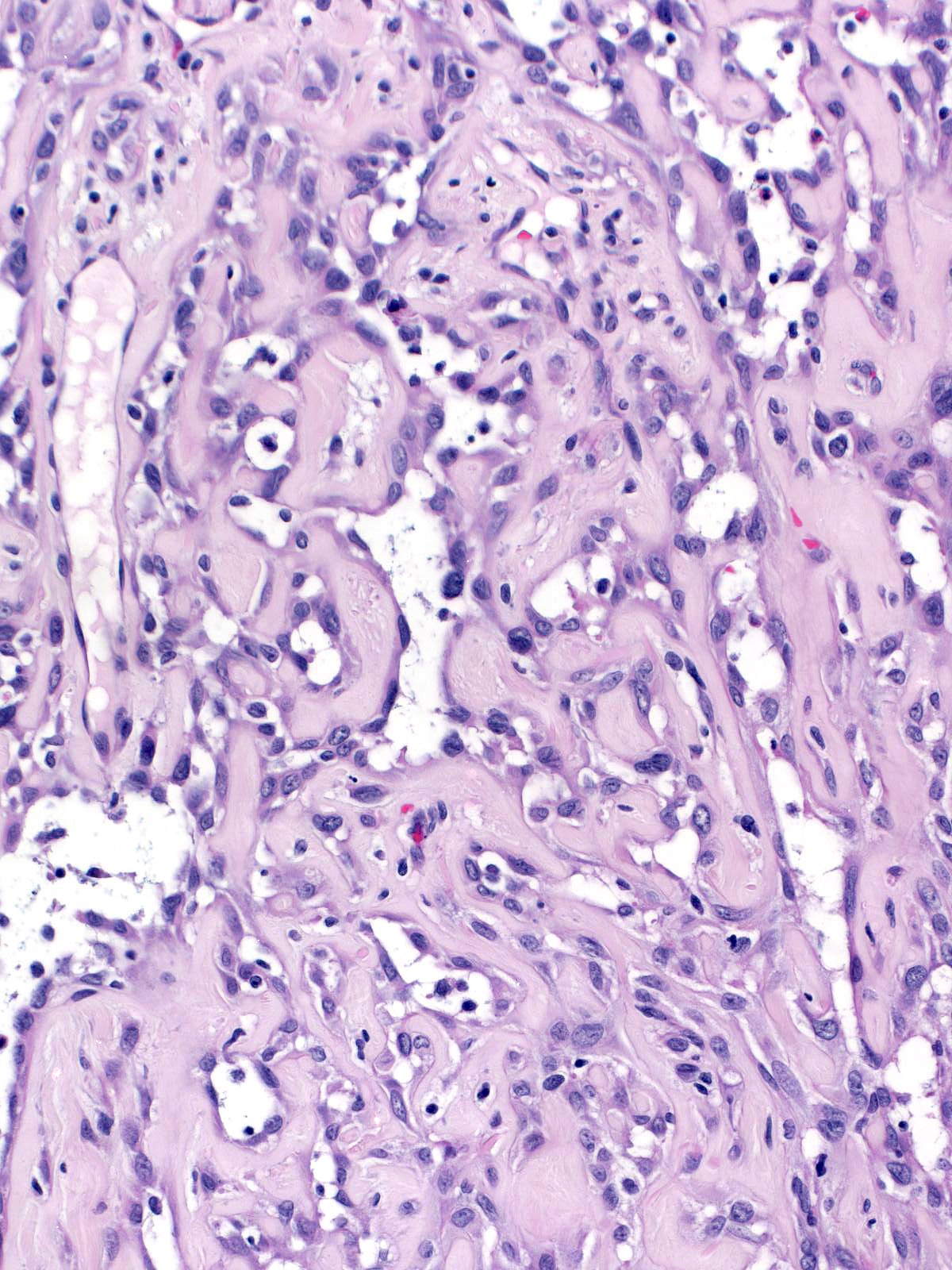
The presence of abundant extracellular matrix characterizes the second common type of metaplastic carcinoma, matrix-producing carcinoma. In most cases, the epithelial nature of the neoplastic cells appears obvious.
These carcinomas consist of small, rounded or polygonal cells forming small loosely cohesive clusters or glands. Less common examples features spindly cells similar to those seen in sarcomas.
 |
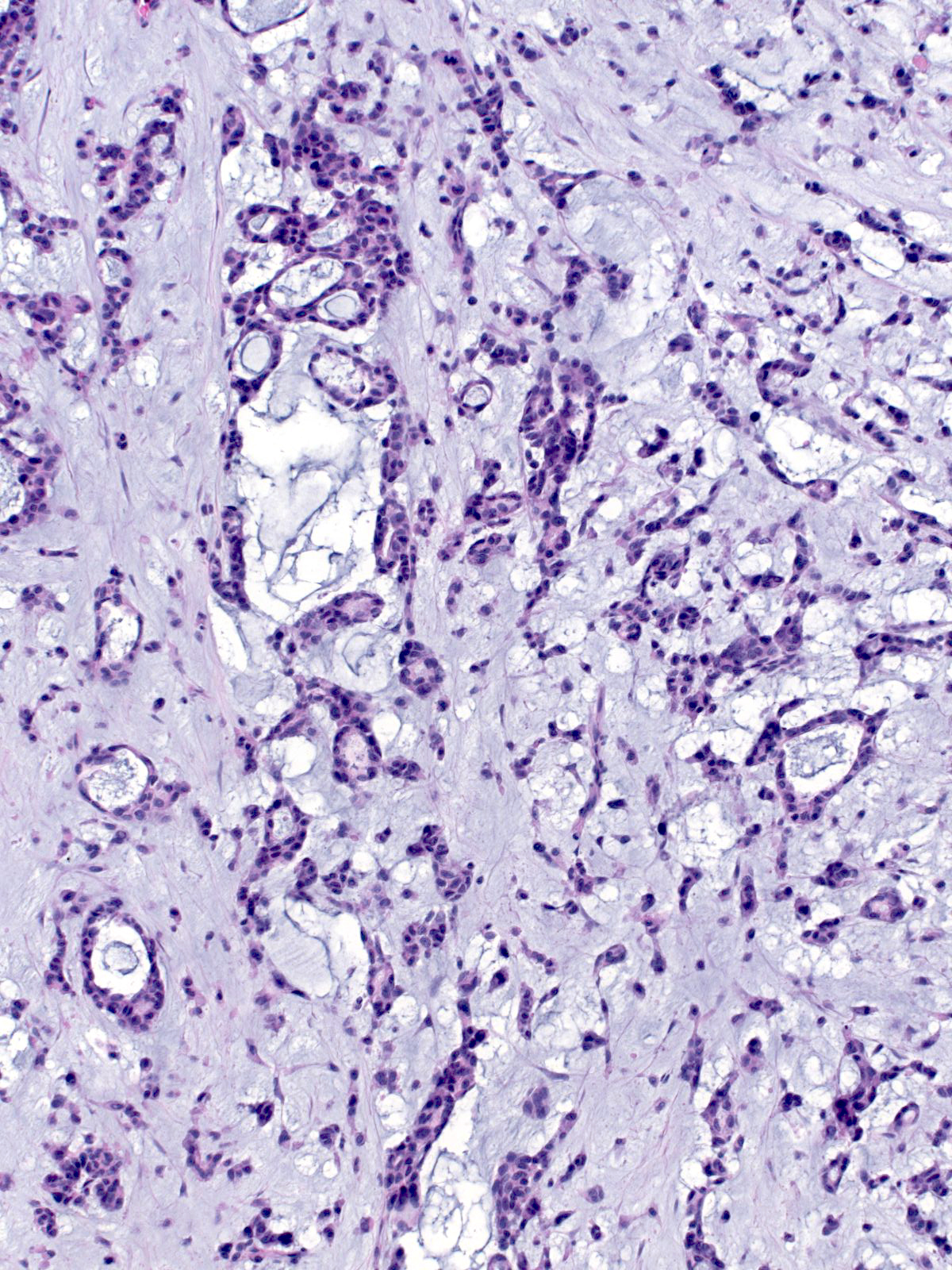 |
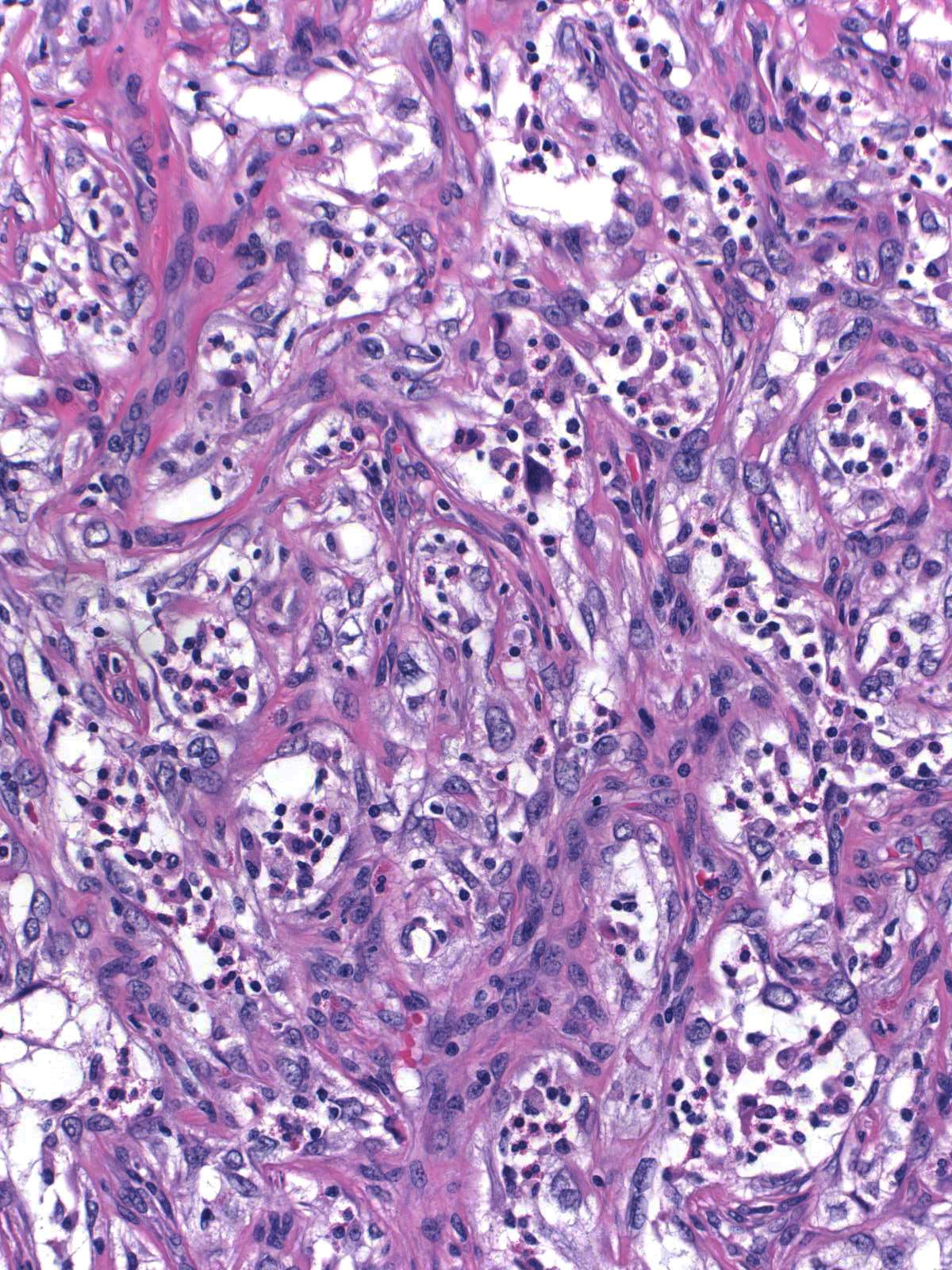
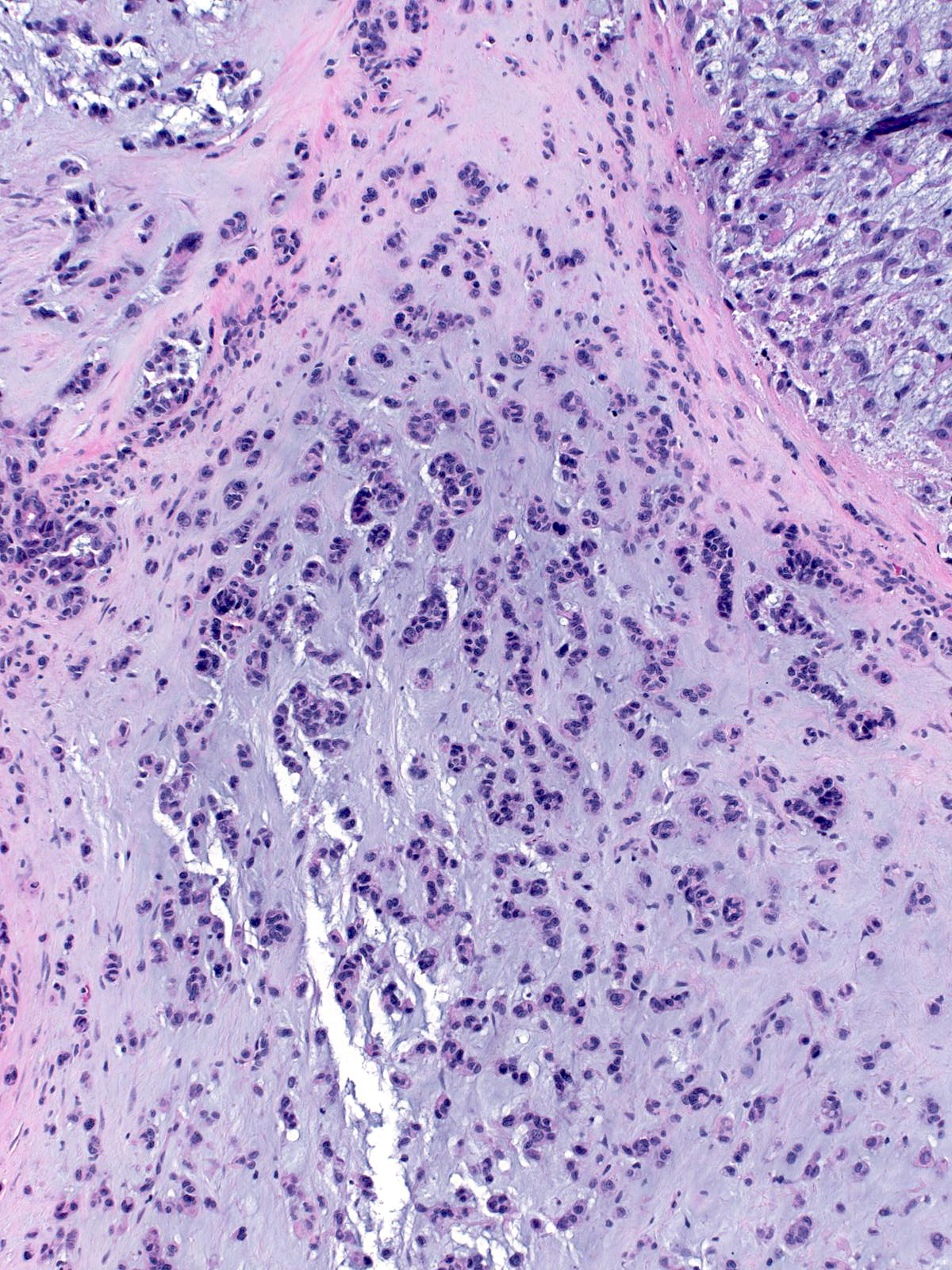
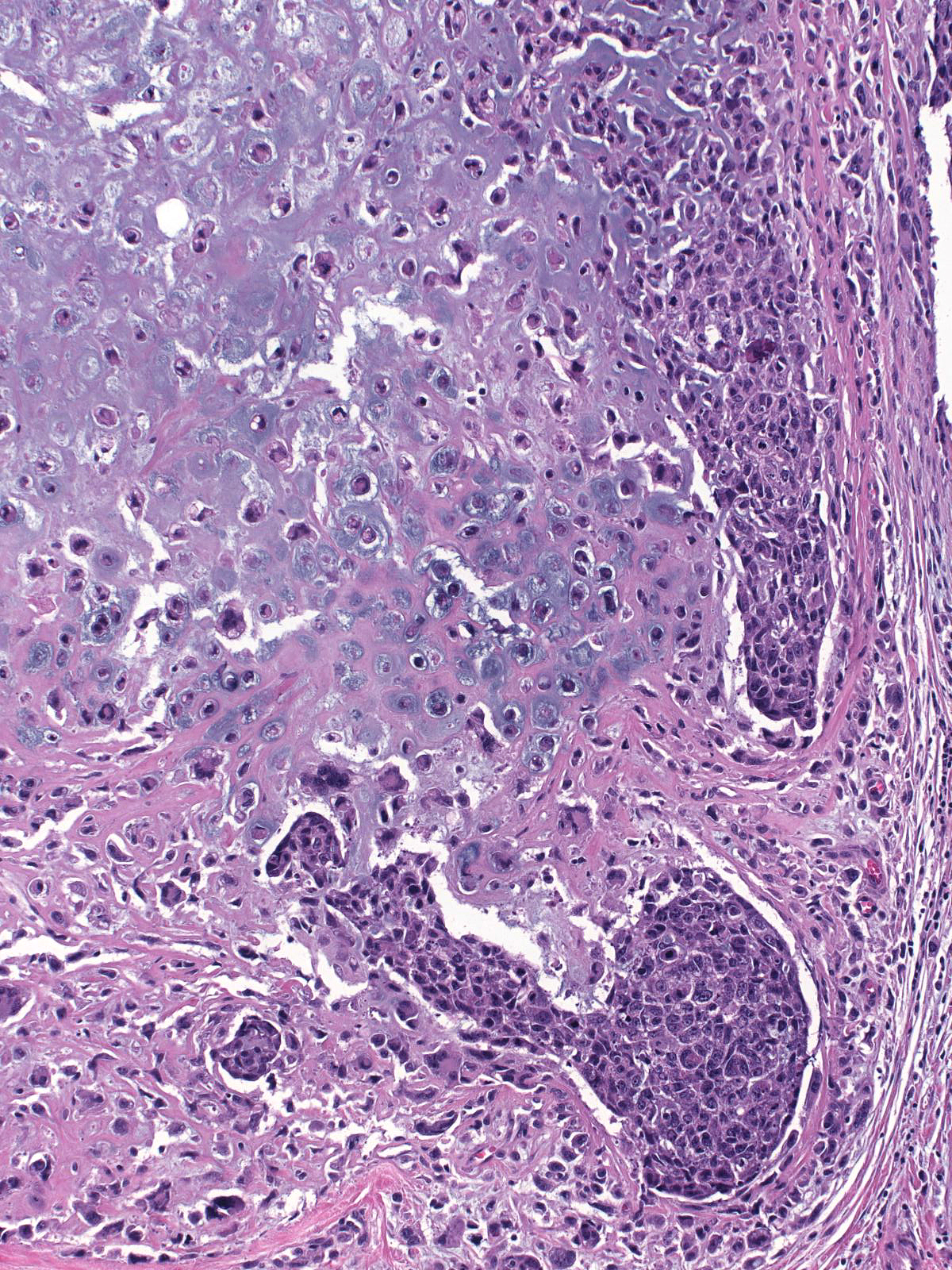
The matrix can appear myxoid (as above), chondroid, or osseous.
 |
 |
| When matrix-producing carcinomas form extensive matrix, they resemble chondrosarcomas or osteosarcomas. |  |