Difference between revisions of "Breast: DE: Ductal Carcinoma In Situ"
(Created page with "== Introduction == {{dxintro|Ductal Carcinoma In Situ|Ductal carcinoma in-situ (DCIS) is a neoplastic proliferation of luminal type ductal epithelial cells.|Ductal carcinoma i...") |
|||
| Line 1: | Line 1: | ||
| + | {{:TOC}} | ||
== Introduction == | == Introduction == | ||
{{dxintro|Ductal Carcinoma In Situ|Ductal carcinoma in-situ (DCIS) is a neoplastic proliferation of luminal type ductal epithelial cells.|Ductal carcinoma in-situ comes to clinical attention because of the presence of calcifications on a mammogram or linear enhancement on MRI. In the uncommon situation in which it produces a pronounced stromal reaction, it can present as a mass. DCIS represents the precursor to invasive ductal carcinoma and usually leads to treatment of the entire involved breast (mastectomy or excision and irradiation). Oncologists usually also recommend hormonal therapy to reduce the risk of developing carcinoma in the contralateral breast.<br>When a core biopsy reveals ductal carcinoma in-situ, a surgeon will typically carry out an excision of the targeted area and marginal tissue. If the radiological or the pathological findings indicate extensive involvement of the breast and in certain other circumstances, the surgeon will recommend a mastectomy and sentinel node excision rather than an excision.<br>Current thinking based on morphological, clinical, and genetic studies asserts that the low-grade and high-grade forms of ductal carcinoma in-situ represent distinct biological entities whose morphological precursors and genetic aberrations do not overlap.|Low-grade DCIS does not usually exhibit macroscopic findings. Transected ducts of high-grade DCIS may exude yellow-white, granular or pasty material (comedonecrosis), corresponding to necrotic carcinoma cells in the duct lumen. Calcifications associated with DCIS may impart a granular texture.|Expansive proliferation of polarized, atypical, slightly dishesive epithelial cells characterizes DCIS.|Usual ductal hyperplasia (highly cohesive, nonpolarized cells), atypical ductal hyperplasia (typically low-grade, less expansive), lobular carcinoma in-situ (dishesive, nonpolarized cells)|Although the cellular features of ductal carcinoma in-situ vary from case to case and can differ somewhat within cases, four alterations represent consistent findings: cellular polarization, cellular enlargement, cytological atypia, and architectural atypia.|Precursor.jpg|Ductal carcinoma in-situ (top) gives rise | {{dxintro|Ductal Carcinoma In Situ|Ductal carcinoma in-situ (DCIS) is a neoplastic proliferation of luminal type ductal epithelial cells.|Ductal carcinoma in-situ comes to clinical attention because of the presence of calcifications on a mammogram or linear enhancement on MRI. In the uncommon situation in which it produces a pronounced stromal reaction, it can present as a mass. DCIS represents the precursor to invasive ductal carcinoma and usually leads to treatment of the entire involved breast (mastectomy or excision and irradiation). Oncologists usually also recommend hormonal therapy to reduce the risk of developing carcinoma in the contralateral breast.<br>When a core biopsy reveals ductal carcinoma in-situ, a surgeon will typically carry out an excision of the targeted area and marginal tissue. If the radiological or the pathological findings indicate extensive involvement of the breast and in certain other circumstances, the surgeon will recommend a mastectomy and sentinel node excision rather than an excision.<br>Current thinking based on morphological, clinical, and genetic studies asserts that the low-grade and high-grade forms of ductal carcinoma in-situ represent distinct biological entities whose morphological precursors and genetic aberrations do not overlap.|Low-grade DCIS does not usually exhibit macroscopic findings. Transected ducts of high-grade DCIS may exude yellow-white, granular or pasty material (comedonecrosis), corresponding to necrotic carcinoma cells in the duct lumen. Calcifications associated with DCIS may impart a granular texture.|Expansive proliferation of polarized, atypical, slightly dishesive epithelial cells characterizes DCIS.|Usual ductal hyperplasia (highly cohesive, nonpolarized cells), atypical ductal hyperplasia (typically low-grade, less expansive), lobular carcinoma in-situ (dishesive, nonpolarized cells)|Although the cellular features of ductal carcinoma in-situ vary from case to case and can differ somewhat within cases, four alterations represent consistent findings: cellular polarization, cellular enlargement, cytological atypia, and architectural atypia.|Precursor.jpg|Ductal carcinoma in-situ (top) gives rise | ||
Revision as of 18:14, August 27, 2019
Contents
Introduction
|
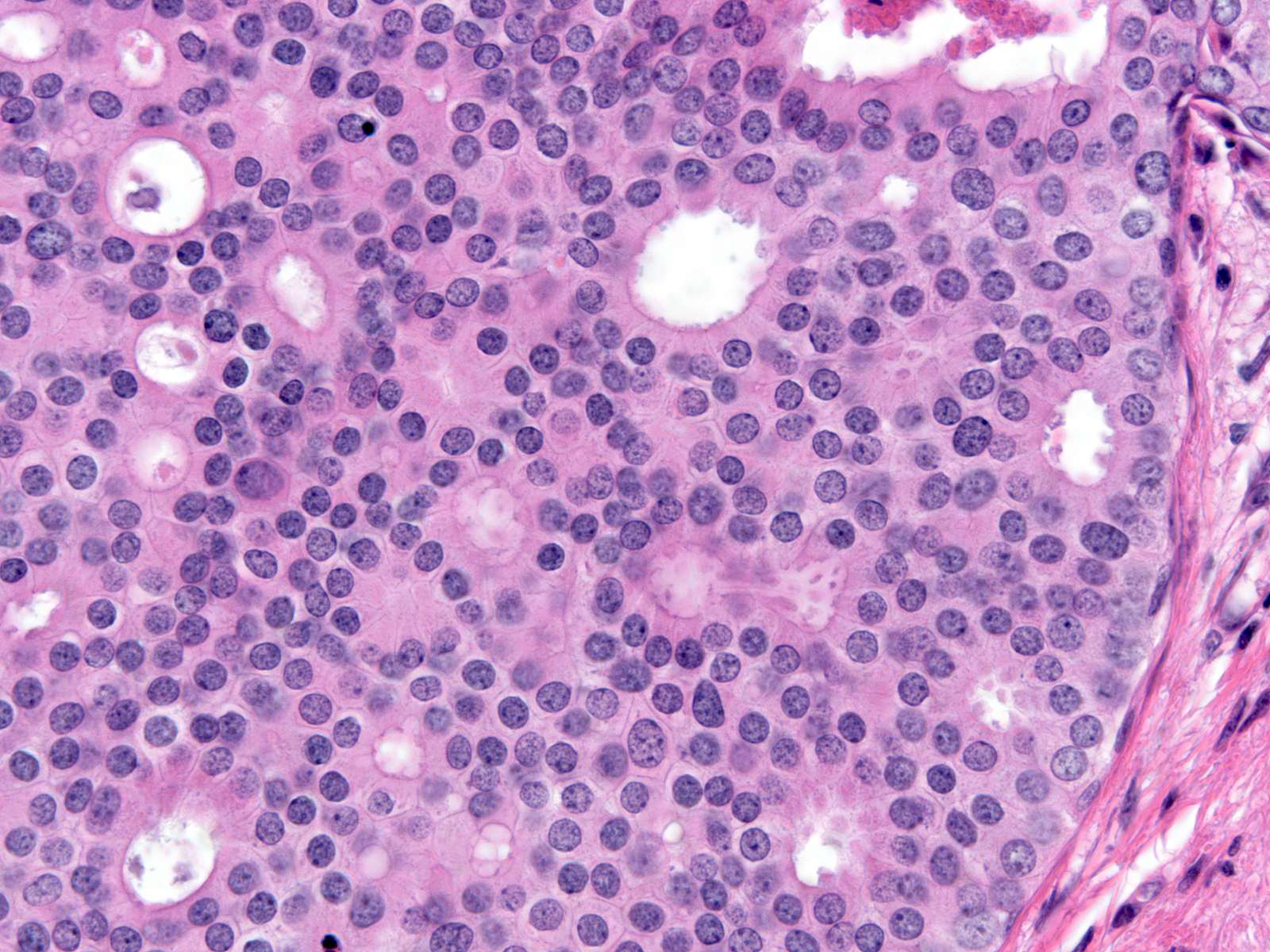
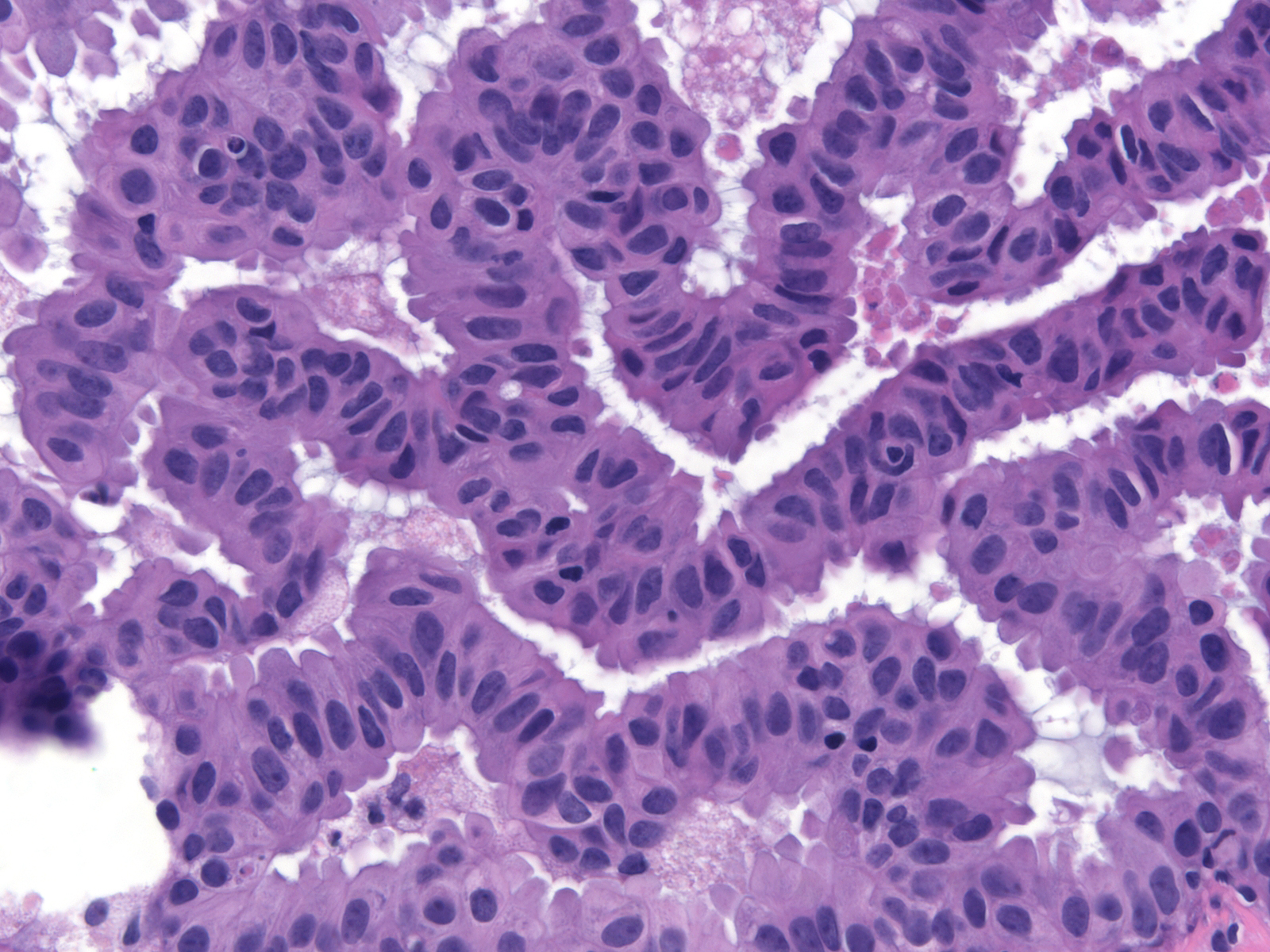
Definition: Ductal carcinoma in-situ (DCIS) is a neoplastic proliferation of luminal type ductal epithelial cells. Clinical Significance: Ductal carcinoma in-situ comes to clinical attention because of the presence of calcifications on a mammogram or linear enhancement on MRI. In the uncommon situation in which it produces a pronounced stromal reaction, it can present as a mass. DCIS represents the precursor to invasive ductal carcinoma and usually leads to treatment of the entire involved breast (mastectomy or excision and irradiation). Oncologists usually also recommend hormonal therapy to reduce the risk of developing carcinoma in the contralateral breast. Gross Findings: Low-grade DCIS does not usually exhibit macroscopic findings. Transected ducts of high-grade DCIS may exude yellow-white, granular or pasty material (comedonecrosis), corresponding to necrotic carcinoma cells in the duct lumen. Calcifications associated with DCIS may impart a granular texture. Microscopic Findings: Expansive proliferation of polarized, atypical, slightly dishesive epithelial cells characterizes DCIS. Differential Diagnosis: Usual ductal hyperplasia (highly cohesive, nonpolarized cells), atypical ductal hyperplasia (typically low-grade, less expansive), lobular carcinoma in-situ (dishesive, nonpolarized cells) Discussion: Although the cellular features of ductal carcinoma in-situ vary from case to case and can differ somewhat within cases, four alterations represent consistent findings: cellular polarization, cellular enlargement, cytological atypia, and architectural atypia. |
 |
Cellular Polarization
The cells of DCIS display the phenomenon of cellular polarization, a fundamental characteristic of normal epithelial cells. We recognize polarization by the location of the nucleus at one end of the cell (referred to as the basal pole) and the accumulation of cytoplasm at the opposite end (referred to as the apical cytoplasmic compartment). Normal ductal epithelial cells rely on signals associated with the basement membrane to establish the orientation needed to achieve polarity. The ability of ductal carcinoma cells to establish polarity far from the basement membrane differentiates these malignant cells from normal mammary cells and from neoplastic lobular cells.
{
 |
 |