Difference between revisions of "mgh:breast-Radial Scar"
| Line 2: | Line 2: | ||
{{:TOC}} | {{:TOC}} | ||
<br> | <br> | ||
| − | {{dxintro|Radial Scar|Radial scar (RADS), also referred to as complex sclerosing lesion, is a benign sclerosing lesion with a characteristic stellate shape and targetoid arrangement.|Radial scars present as palpable masses or stellate imaging abnormalities. The clinical and radiographic findings resemble those of an invasive carcinoma. Radial scars do not give rise to invasive carcinomas, nor do they indicate a heightened risk for the development of carcinoma.|When a core biopsy reveals a radial scar, a surgeon will usually carry out an excision of the targeted area to exclude the presence of an atypical epithelial proliferation or a misdiagnosed invasive carcinoma.|The typical radial scar forms a poorly defined, spiculated, firm to hard mass of white tissue.|Radial scars consist of a region of parenchyma loss and scarring with retraction and distortion of the surrounding tissue. Most have a symmetrical shape and a targetoid organization featuring a fibroelastotic center and proliferative periphery.|Invasive ductal carcinoma (no targetoid organization, extension of glands beyond altered stroma, no evidence of myoepithelial cells, associated ductal carcinoma in-situ) | + | {{dxintro|Radial Scar|Radial scar (RADS), also referred to as complex sclerosing lesion, is a benign sclerosing lesion with a characteristic stellate shape and targetoid arrangement.|Radial scars present as palpable masses or stellate imaging abnormalities. The clinical and radiographic findings resemble those of an invasive carcinoma. Radial scars do not give rise to invasive carcinomas, nor do they indicate a heightened risk for the development of carcinoma.|When a core biopsy reveals a radial scar, a surgeon will usually carry out an excision of the targeted area to exclude the presence of an atypical epithelial proliferation or a misdiagnosed invasive carcinoma.|The typical radial scar forms a poorly defined, spiculated, firm to hard mass of white tissue.|Radial scars consist of a region of parenchyma loss and scarring with retraction and distortion of the surrounding tissue. Most have a symmetrical shape and a targetoid organization featuring a fibroelastotic center and proliferative periphery.|Invasive ductal carcinoma (no targetoid organization, extension of glands beyond altered stroma, no evidence of myoepithelial cells, associated ductal carcinoma in-situ). Typical, well developed radial scars have a symmetrical, zonal, targetoid appearance. The center, termed the nidus, demonstrates scarring and glandular entrapment, and the surrounding zone, termed the corona, shows proliferative glandular and epithelial changes.|15-1 Corona 2-2.jpg|Radial scars have a spiculated appearance because of central parenchymal loss and distortion of the surrounding tissue.}} |
== Zonal Architecture == | == Zonal Architecture == | ||
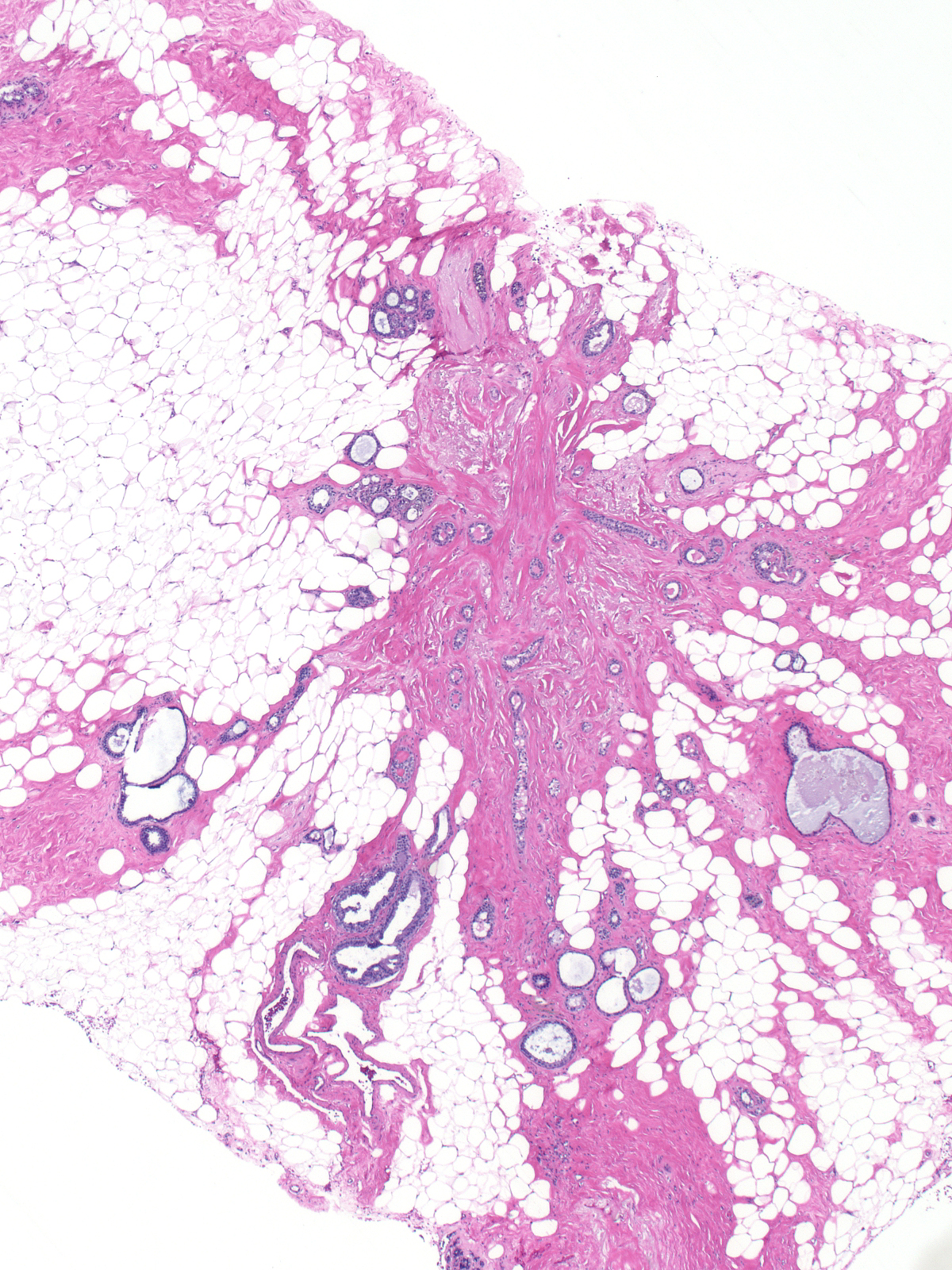
{{img1|The nidus (central circle) demonstrates fibroelastotic scarring and entrapment of glands. The corona (outer circle) displays glandular and epithelial proliferation. Most often, the corona also exhibits cystic change.|15-2 Targetoid.jpg}} | {{img1|The nidus (central circle) demonstrates fibroelastotic scarring and entrapment of glands. The corona (outer circle) displays glandular and epithelial proliferation. Most often, the corona also exhibits cystic change.|15-2 Targetoid.jpg}} | ||
Latest revision as of 09:09, July 17, 2020
|
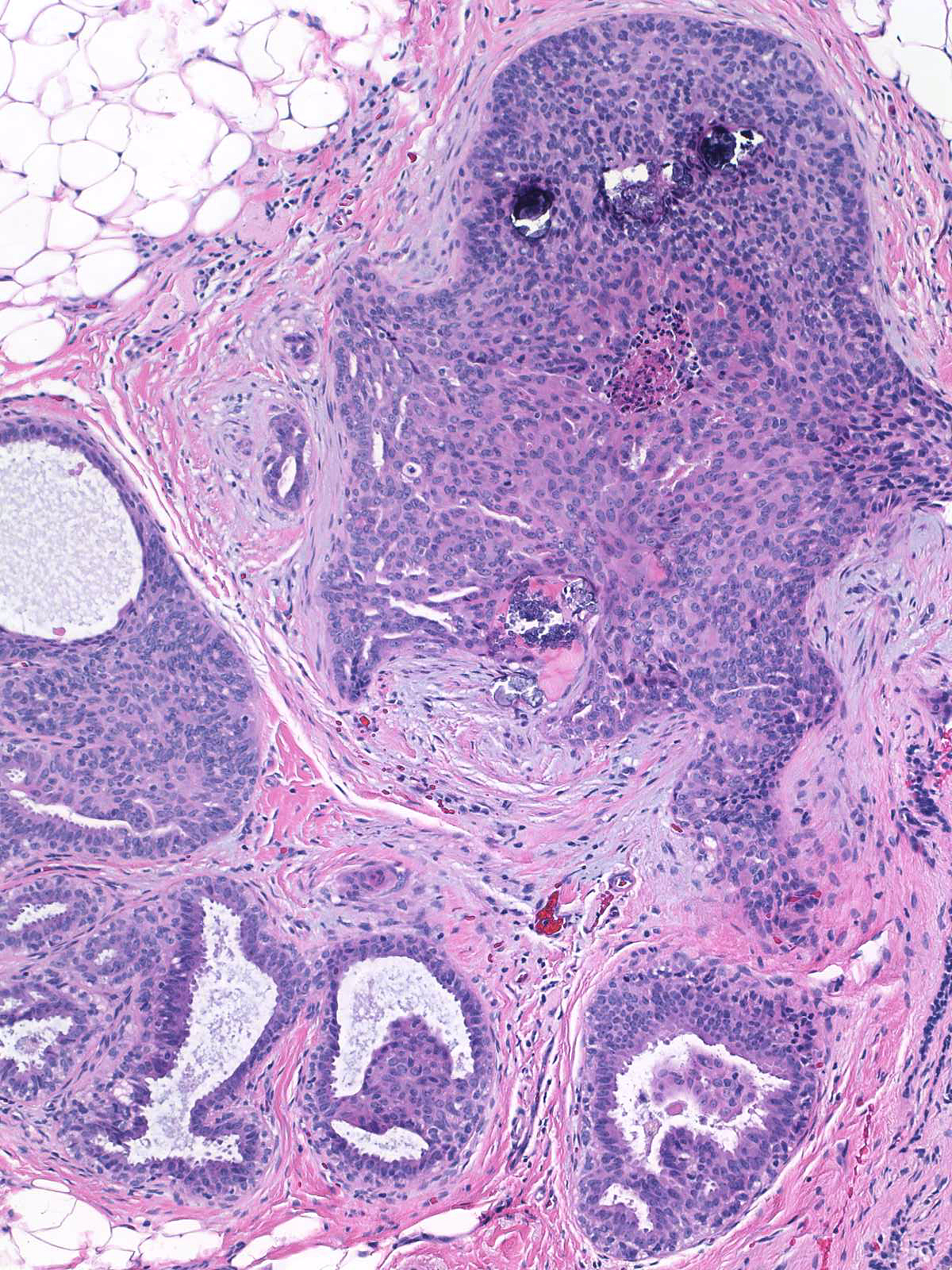
Definition: Radial scar (RADS), also referred to as complex sclerosing lesion, is a benign sclerosing lesion with a characteristic stellate shape and targetoid arrangement. Clinical Significance: Radial scars present as palpable masses or stellate imaging abnormalities. The clinical and radiographic findings resemble those of an invasive carcinoma. Radial scars do not give rise to invasive carcinomas, nor do they indicate a heightened risk for the development of carcinoma. Gross Findings: When a core biopsy reveals a radial scar, a surgeon will usually carry out an excision of the targeted area to exclude the presence of an atypical epithelial proliferation or a misdiagnosed invasive carcinoma. Microscopic Findings: The typical radial scar forms a poorly defined, spiculated, firm to hard mass of white tissue. Differential Diagnosis: Radial scars consist of a region of parenchyma loss and scarring with retraction and distortion of the surrounding tissue. Most have a symmetrical shape and a targetoid organization featuring a fibroelastotic center and proliferative periphery. Discussion: Invasive ductal carcinoma (no targetoid organization, extension of glands beyond altered stroma, no evidence of myoepithelial cells, associated ductal carcinoma in-situ). Typical, well developed radial scars have a symmetrical, zonal, targetoid appearance. The center, termed the nidus, demonstrates scarring and glandular entrapment, and the surrounding zone, termed the corona, shows proliferative glandular and epithelial changes. |
 |
Zonal Architecture
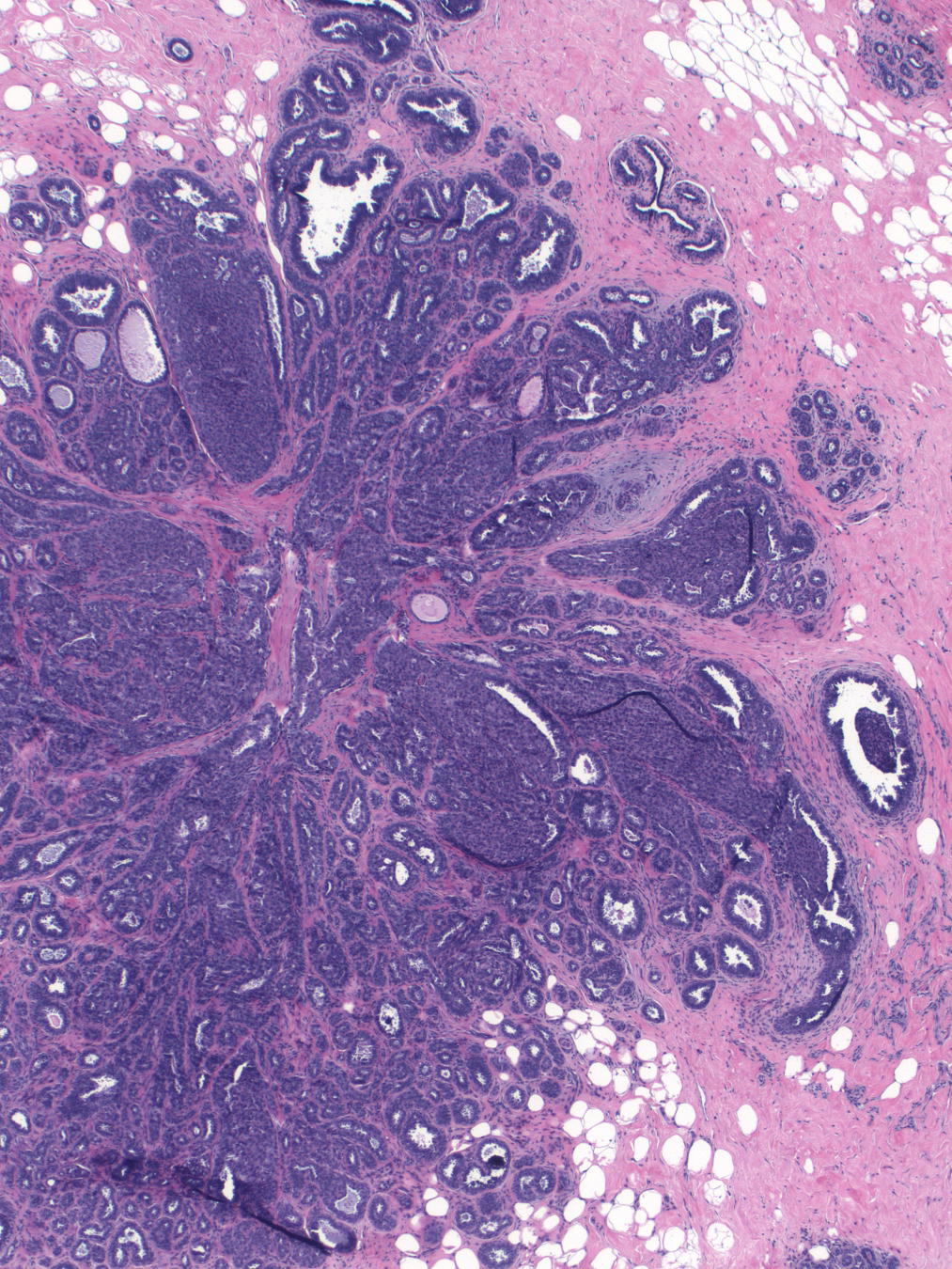
| The nidus (central circle) demonstrates fibroelastotic scarring and entrapment of glands. The corona (outer circle) displays glandular and epithelial proliferation. Most often, the corona also exhibits cystic change. | 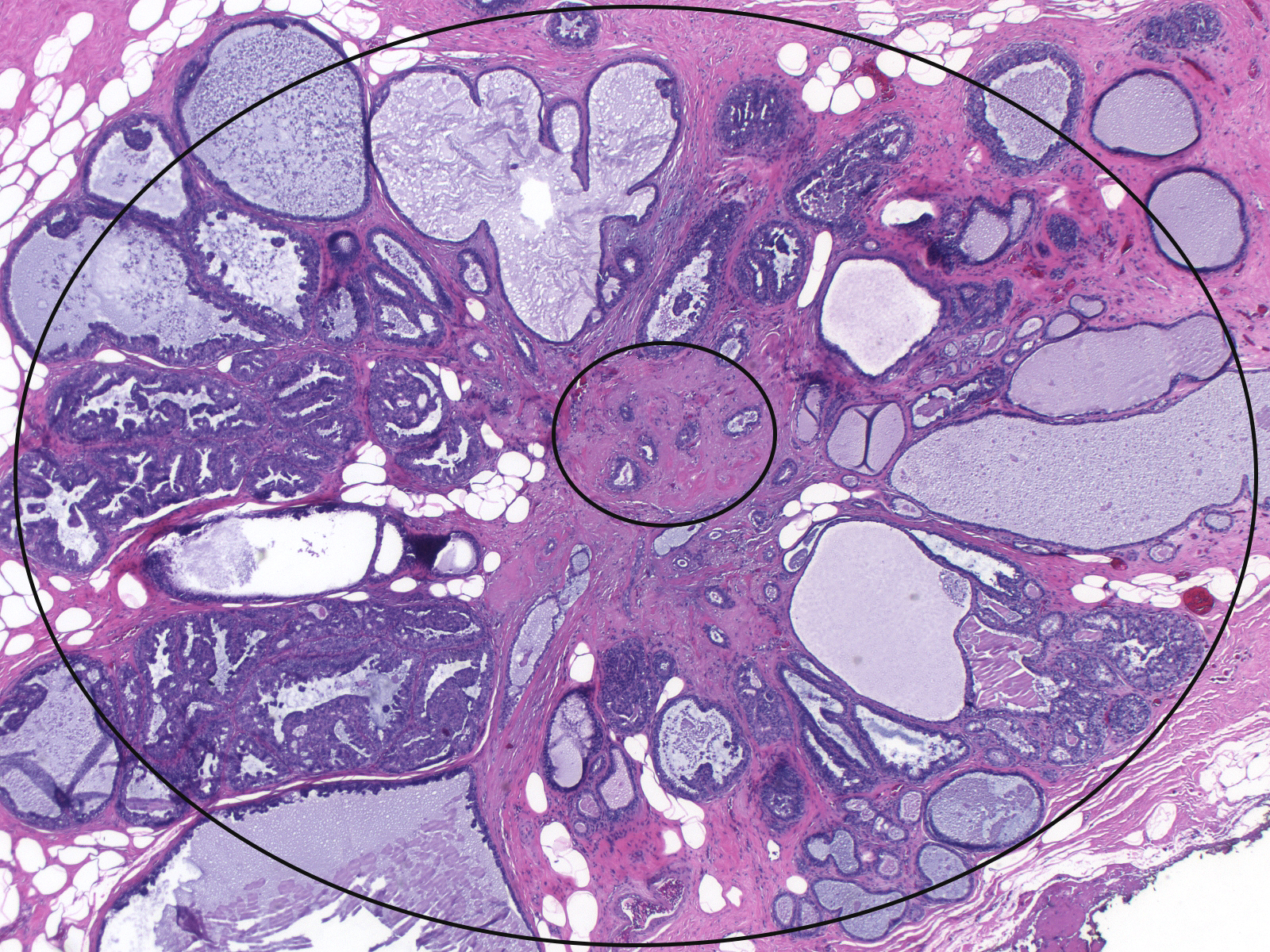 |
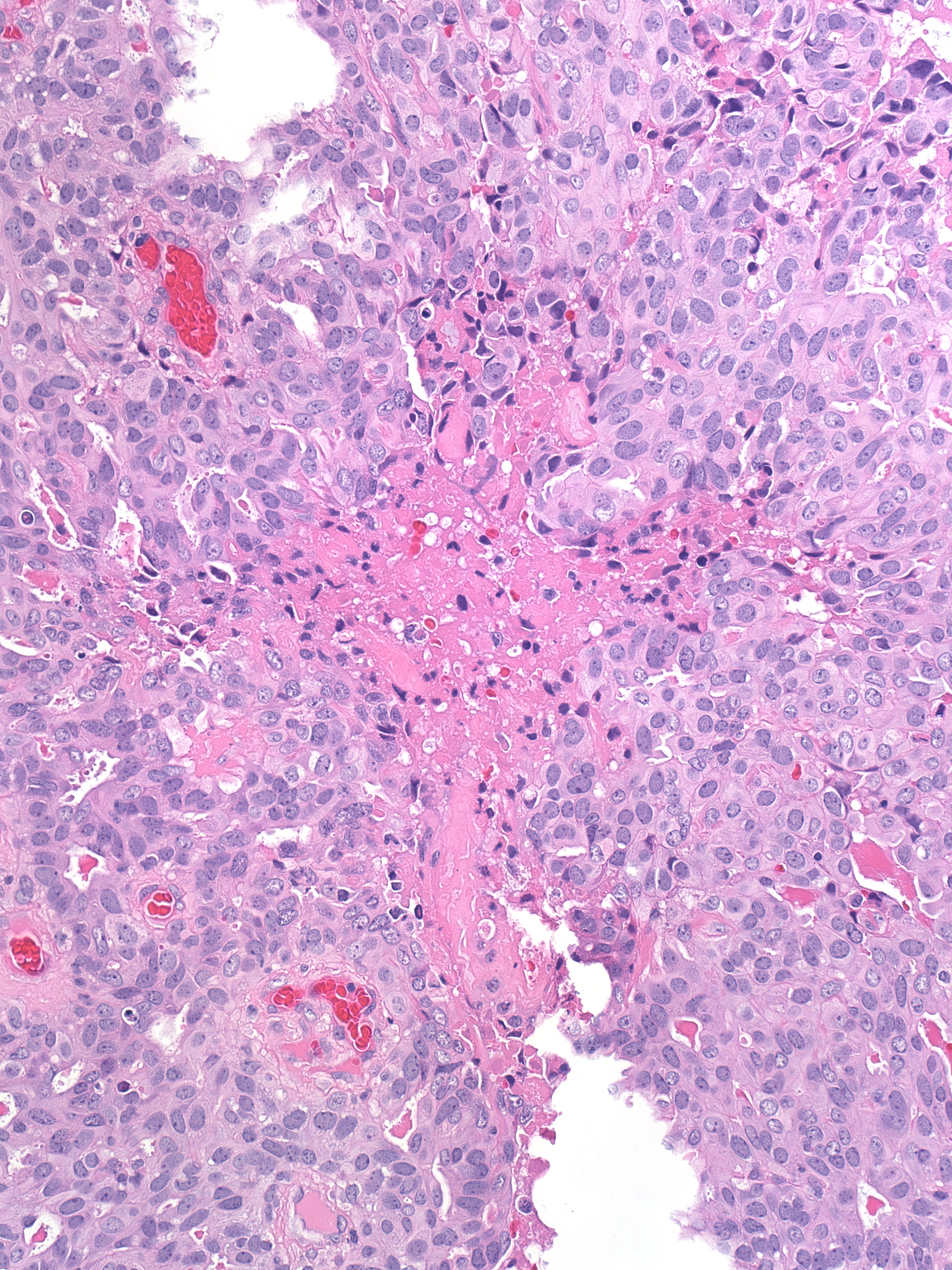
| Here we see a nidus with characteristic small tubular glands irregularly disposed in stroma composed of dense collagen and elastic tissue. | 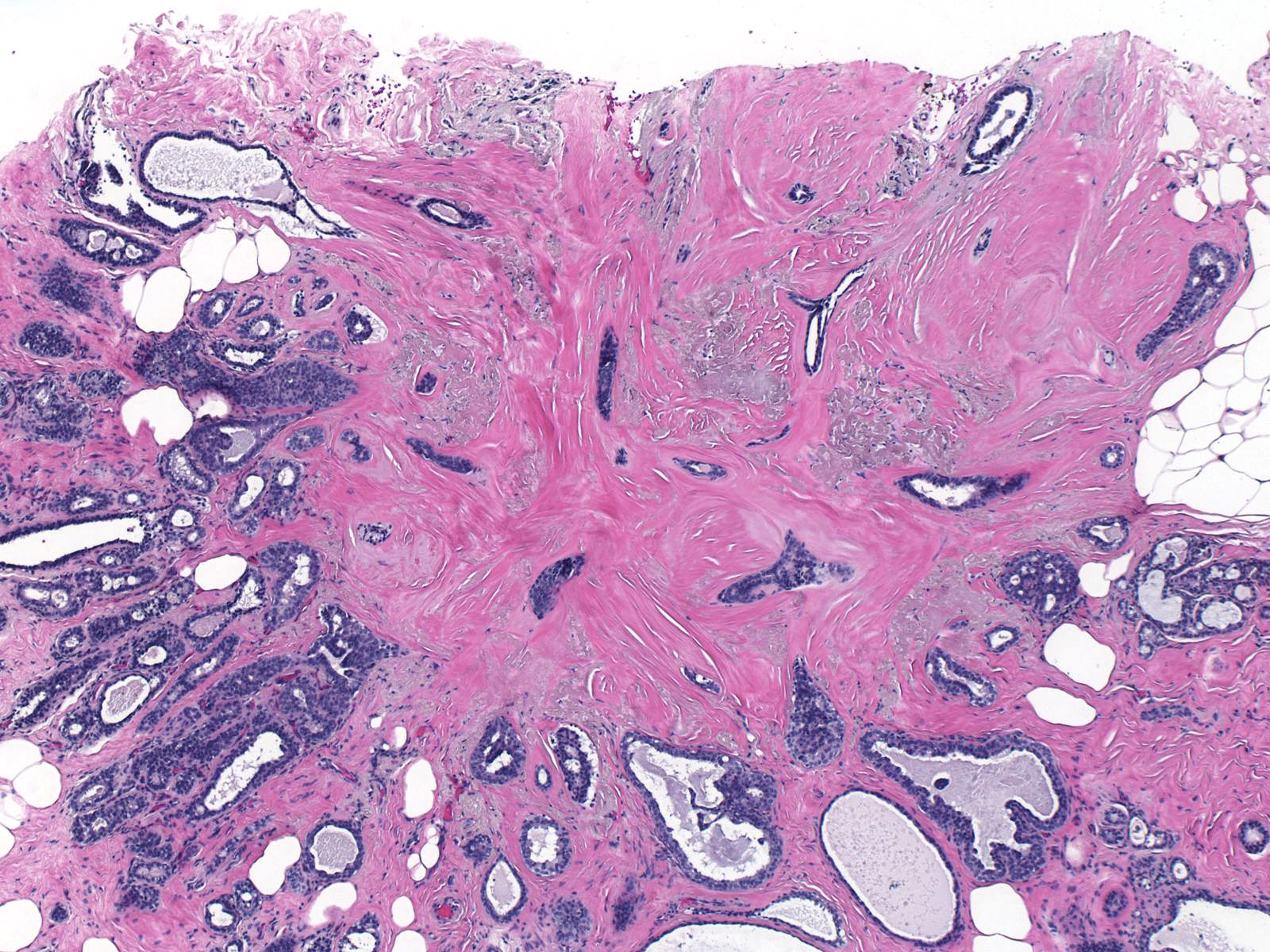 |
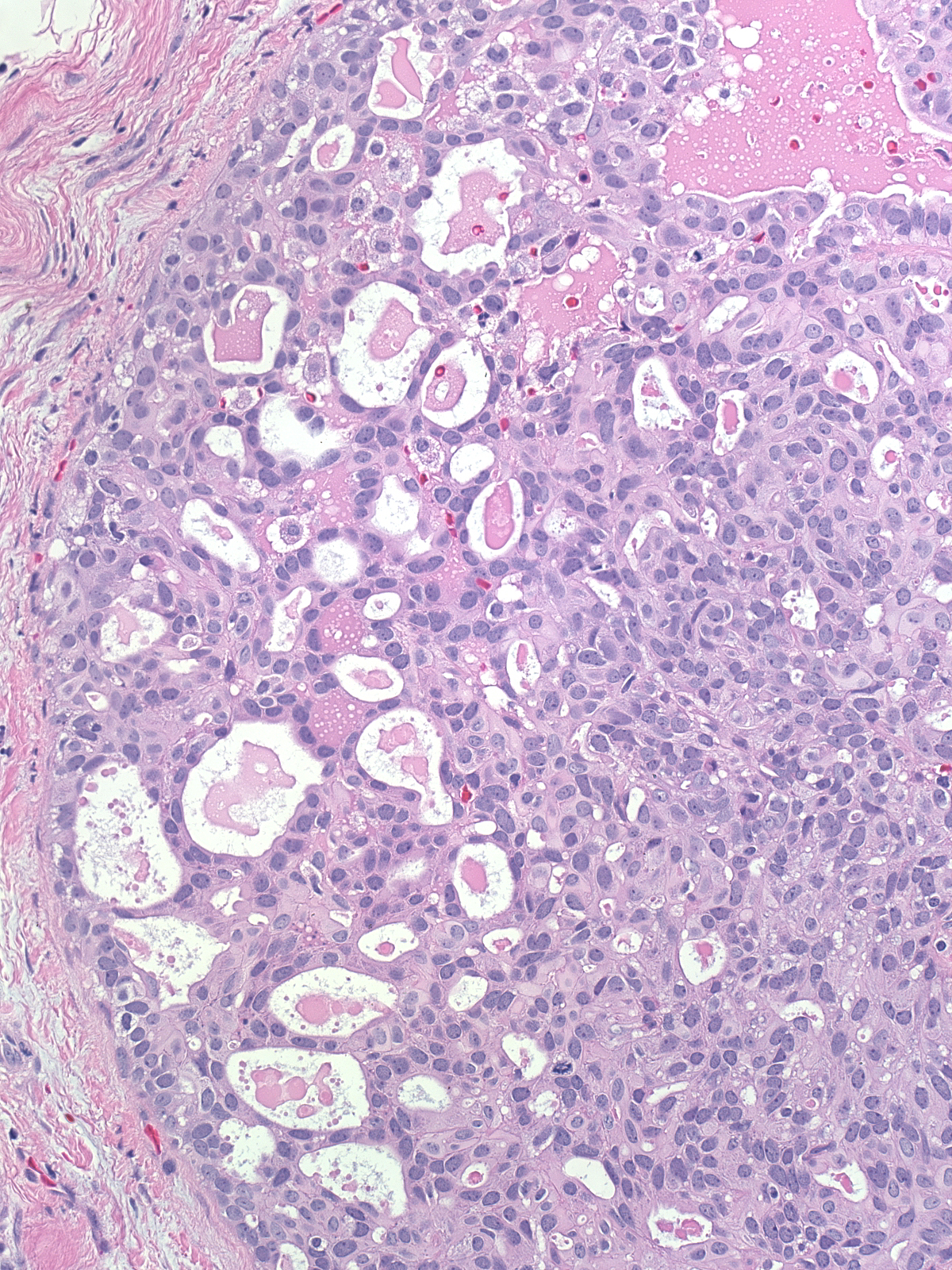
| The glands entrapped in the nidus consist of bland luminal cells enveloped by myoepithelial cells. In rare cases, myoepithelial cells cannot be detected in a few of the glands; however, neighboring similar appearing glands will reassuringly show evidence of myoepithelial cells. | 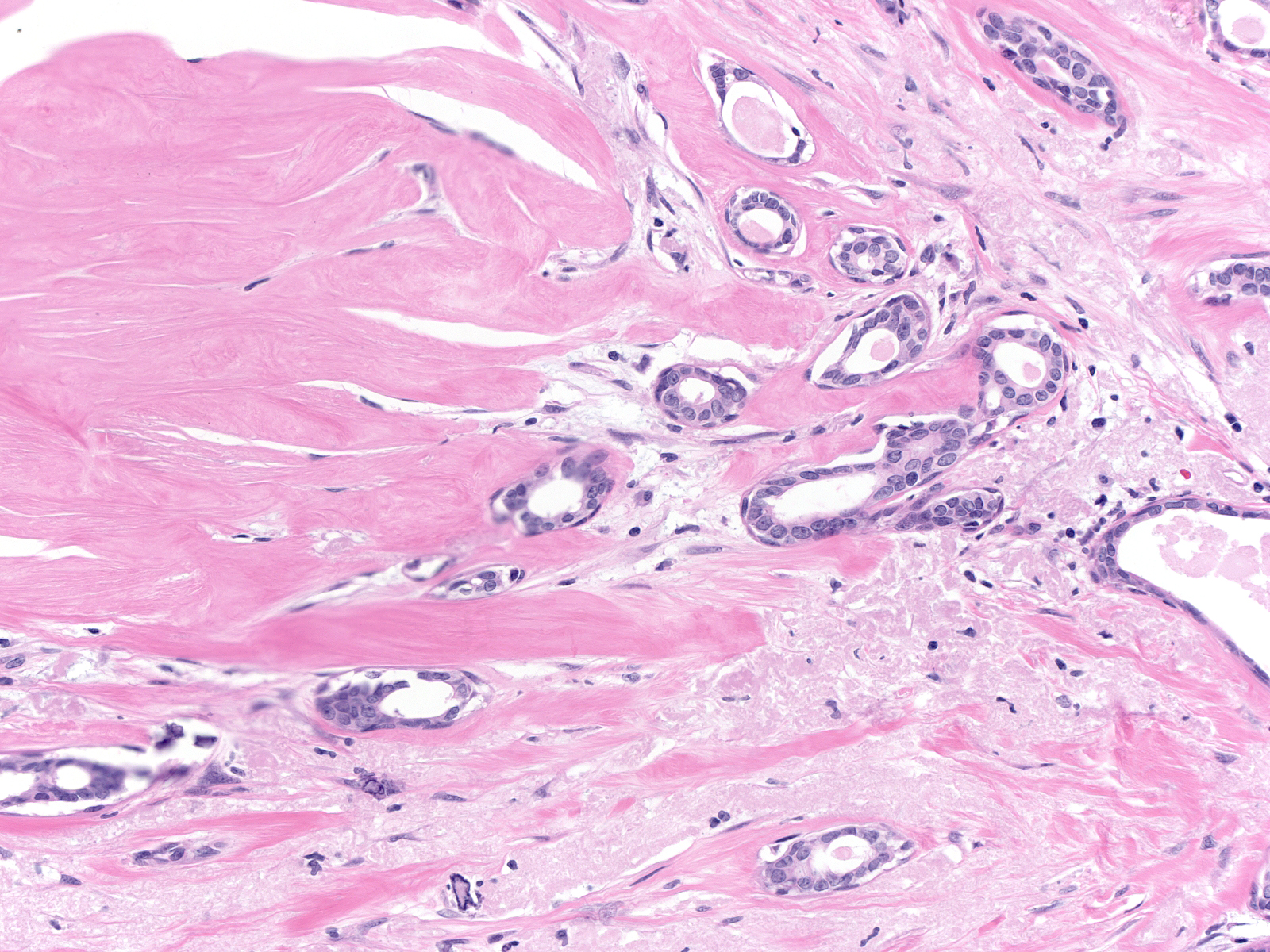 |
| The corona displays any of the common proliferative changes: adenosis, cyst formation, ductal hyperplasia, papilloma formation, etc. | 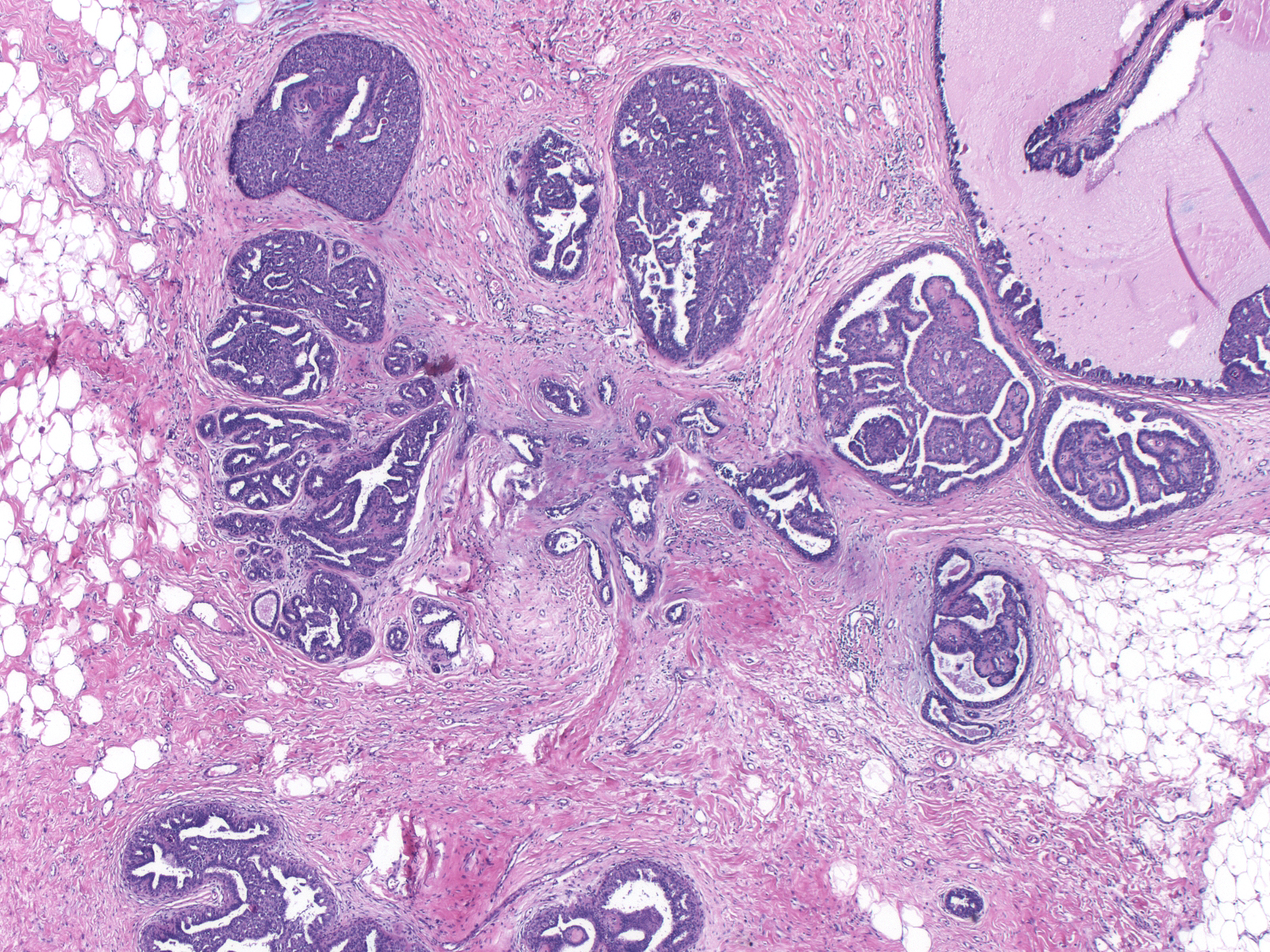 |
Benign hyperplastic ductal cells within the corona of a radial scar can appear slightly larger than those seen in typical usual ductal hyperplasia; they can form spaces that look somewhat cribriform; and they can demonstrate necrosis. These changes do not merit the designation of atypical ductal hyperplasia.
 |
 |
Variations in Architecture
Although one can detect a zonal architecture in most radial scars, the degree of symmetry and the size and shape of the components vary. Some radial scars appear vague and poorly formed, others somewhat flattened. Some of these odd shapes may result from coalescence of adjacent scars.
 |
 |
Some scars appear one-sided.
 |
 |
The size of the nidus varies from unapparent to large.
 |
 |
| The nidus sometimes has a stellate shape with rays of altered stroma extending into the surrounding corona. | 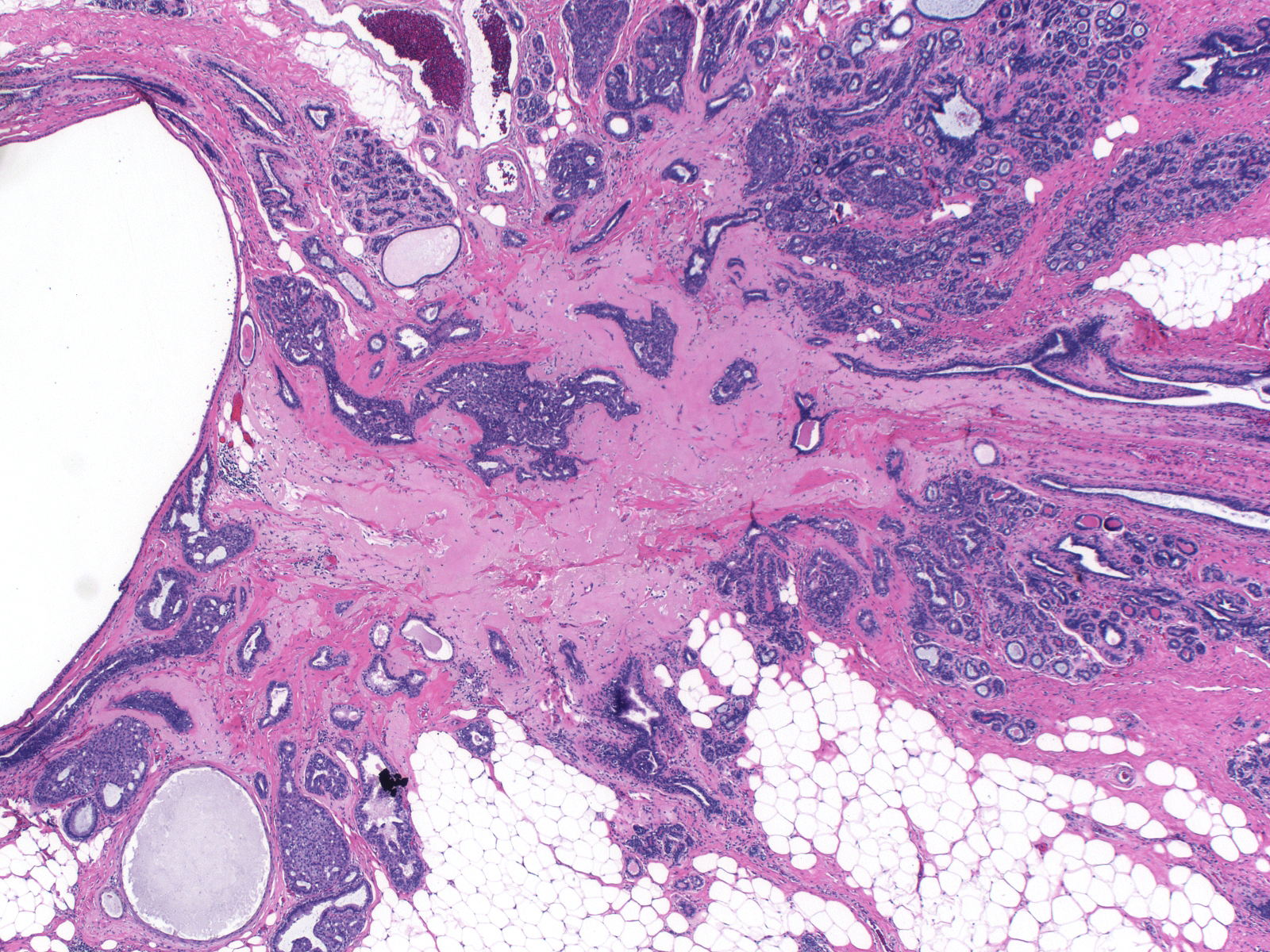 |
The corona also varies in size and shape. Certain scars seem to lack a corona, whereas others consist almost entirely of a corona.
 |
 |
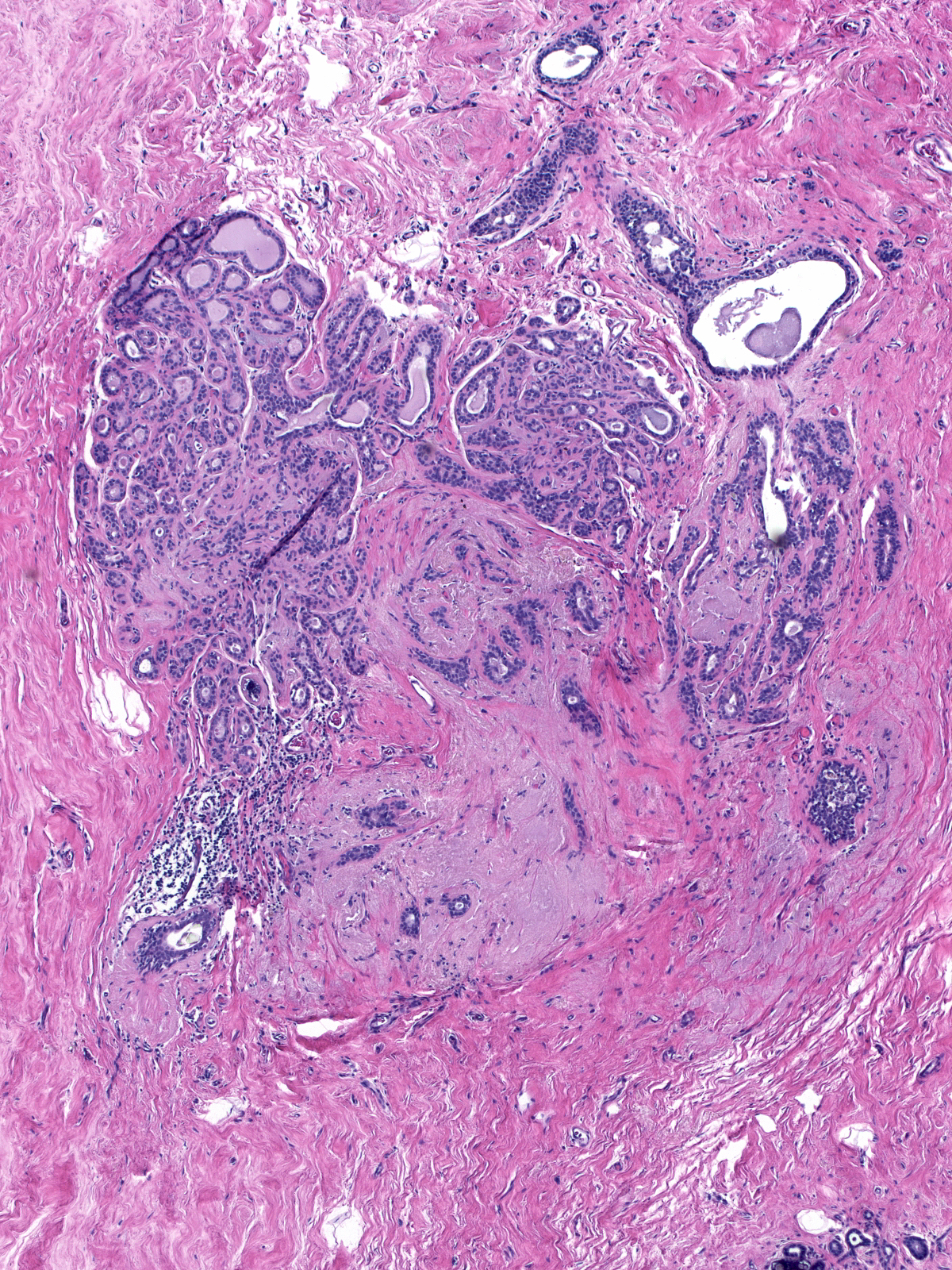
| Whereas the size and shape of a radial scar and its components may vary, one feature remains constant: the distorted glands always sit in altered stroma. |  |
Early Radial Scars
| The morphological features of radial scars in their early phases differ from those of typical radial scars in several ways. For instance, early scars tend to have a more rounded contour compared to the classic spiculated shape of a mature radial scar. | 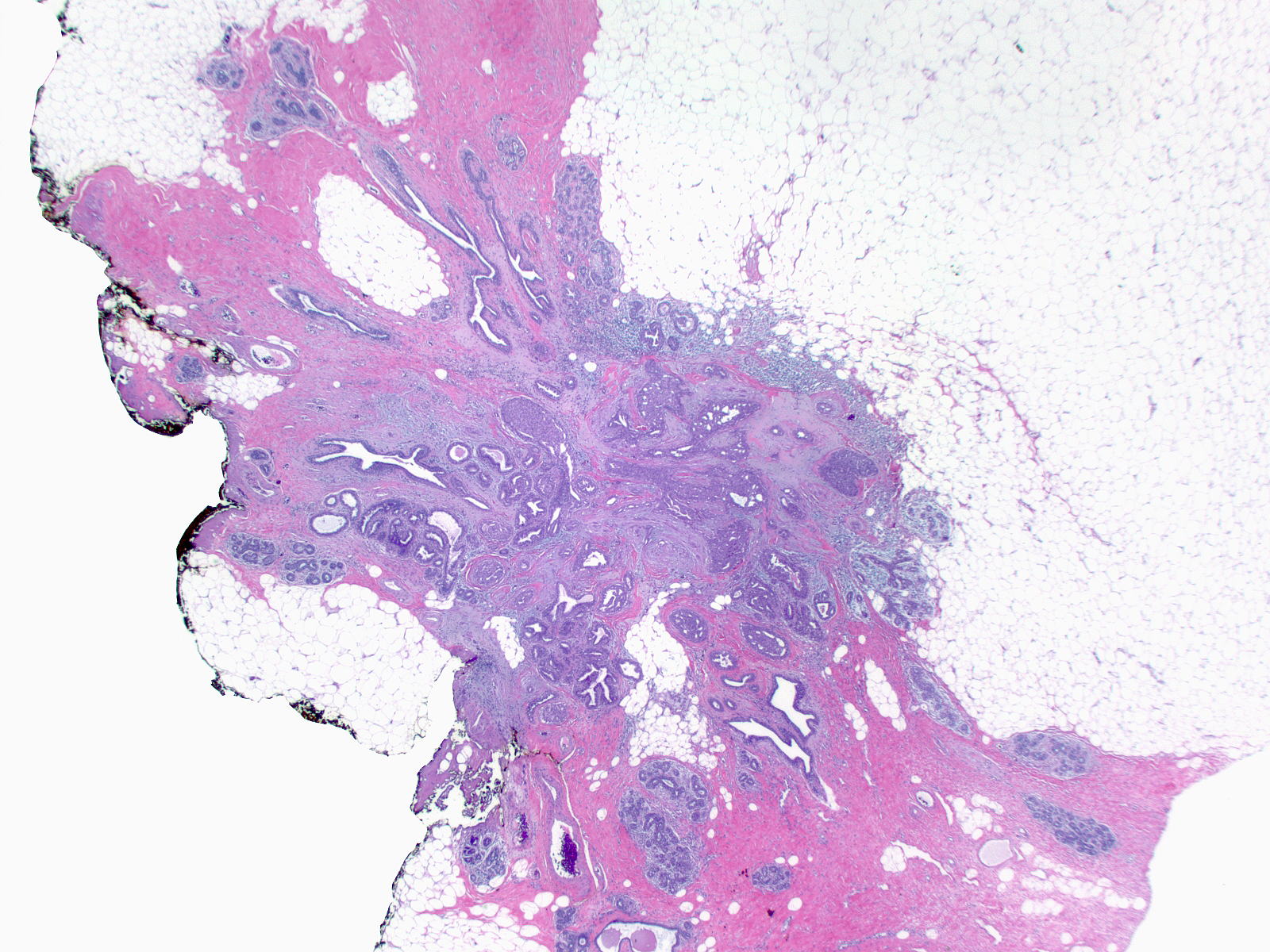 |
| The nidus of an early scar appears somewhat diffuse in contrast with the more compact, well defined mature form. |  |
| The glands can have spindly shapes and poorly developed lumens. | 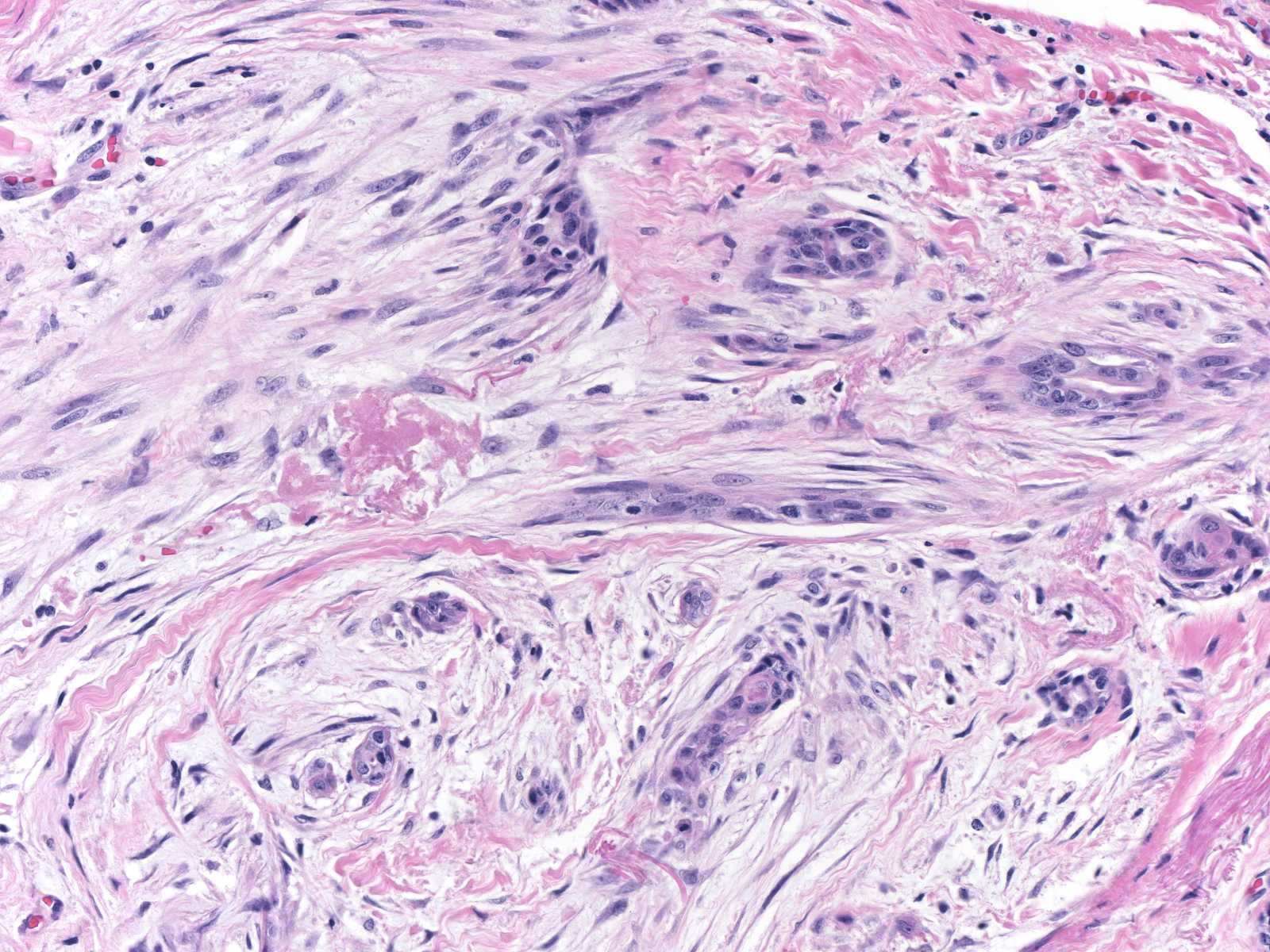 |
| The stroma of the nidus in an early radial scar often consists of numerous fibroblasts sitting in myxoid ground substances rather than dense collagen and elastic tissue.15-21 Early_Stroma.jpg | |
Ductal hyperplasia within the corona of an early radial scar often appears especially florid and can undergo necrosis.
 |
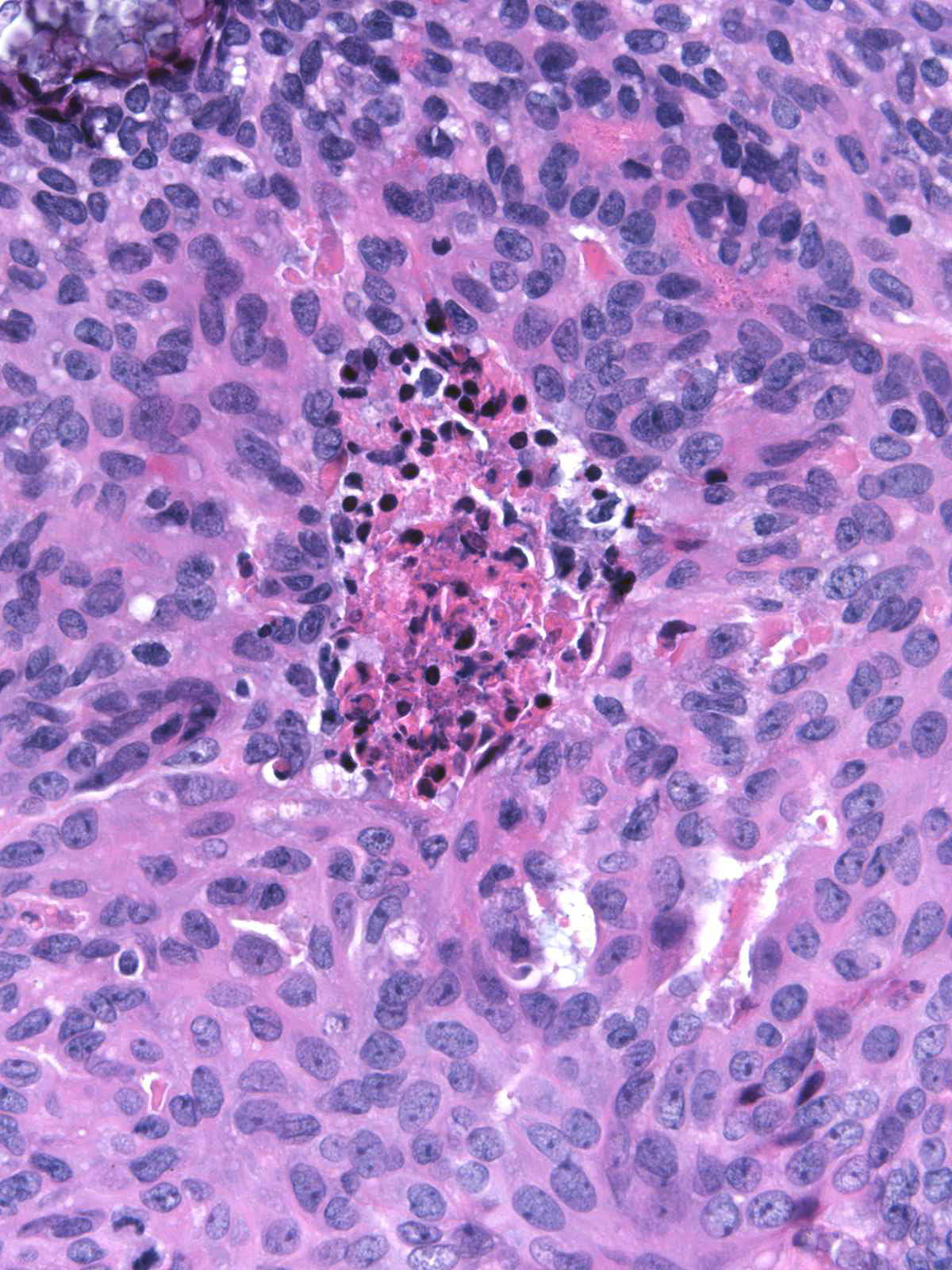 |
| Often helpful in recognizing an early radial scar, lymphocytes tend to cluster at the interface of the nidus and the adjacent parenchyma. |  |