Difference between revisions of "mgh:breast-Sclerosing Adenosis"
| (One intermediate revision by the same user not shown) | |||
| Line 1: | Line 1: | ||
| − | __NOCACHE__ | + | __NOCACHE__ |
{{:TOC}} | {{:TOC}} | ||
| − | == | + | <br> |
| − | + | == Introduction == | |
| − | + | {{dxintro|Sclerosing Adenosis|Sclerosing adenosis is an alteration of pre-existing lobules featuring proliferation of slender tubules (adenosis) and deposition of basement membrane proteins (sclerosis).|Sclerosing adenosis usually does not produce distinctive clinical findings. The lesion can give rise to clustered calcifications, which radiologists usually describe as indeterminate. When foci coalesce to form large nodules, an irregular mass may become apparent either by palpation or by imaging.|Sclerosing adenosis does not usually give rise to macroscopic findings. Large lobules with well developed alterations can present as firm white foci about the size of a grain of sand. The confluence of large regions of sclerosing adenosis gives rise to an ill-defined, firm, white mass referred to as an adenosis tumor.|Examples of sclerosing adenosis demonstrate a proliferation of slender, compressed glandular elements surrounded by extracellular basement membrane proteins. Although the proportions of the glandular proliferation and the matrix production vary from case to case, one must observe both processes to establish the diagnosis of sclerosing adenosis. When examining a small portion of a focus of sclerosing adenosis, one may not be able to appreciate the lobular organization of the process. In this circumstance, one could mistake a focus of sclerosing adenosis for an invasive lobular carcinoma.|Invasive carcinoma (more atypical, infiltrative, less circumscribed)|Sclerosing adenosis originates in the center of normally formed lobules, where the glandular proliferation and matrix deposition surround the intralobular terminal ductule.|16-1 SA_without_TDU-2.jpg|A proliferation of compressed tubules (adenosis) are imbedded in dense eosinophilic material (sclerosis).}} | |
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | When examining a small portion of a focus of sclerosing adenosis, one may not be able to appreciate the lobular organization of the process. In this circumstance, one could mistake a focus of sclerosing adenosis for an invasive lobular carcinoma. | ||
| − | |||
| − | |||
| − | |||
| − | |||
{{img1|Flattened glands and eosinophilic extracellular matrix surround the intralobular terminal ductule in this affected lobule.|16-2 Lobule_20_x.jpg}} | {{img1|Flattened glands and eosinophilic extracellular matrix surround the intralobular terminal ductule in this affected lobule.|16-2 Lobule_20_x.jpg}} | ||
{{img1|Near the center of the lesion, compression of the tubules makes it virtually impossible to identify the lumens of the tubules in most cases.|16-3 High_power_40_x_A_ret.jpg}} | {{img1|Near the center of the lesion, compression of the tubules makes it virtually impossible to identify the lumens of the tubules in most cases.|16-3 High_power_40_x_A_ret.jpg}} | ||
Latest revision as of 09:11, July 17, 2020
Contents
Introduction
|
Definition: Sclerosing adenosis is an alteration of pre-existing lobules featuring proliferation of slender tubules (adenosis) and deposition of basement membrane proteins (sclerosis). Clinical Significance: Sclerosing adenosis usually does not produce distinctive clinical findings. The lesion can give rise to clustered calcifications, which radiologists usually describe as indeterminate. When foci coalesce to form large nodules, an irregular mass may become apparent either by palpation or by imaging. Gross Findings: Sclerosing adenosis does not usually give rise to macroscopic findings. Large lobules with well developed alterations can present as firm white foci about the size of a grain of sand. The confluence of large regions of sclerosing adenosis gives rise to an ill-defined, firm, white mass referred to as an adenosis tumor. Microscopic Findings: Examples of sclerosing adenosis demonstrate a proliferation of slender, compressed glandular elements surrounded by extracellular basement membrane proteins. Although the proportions of the glandular proliferation and the matrix production vary from case to case, one must observe both processes to establish the diagnosis of sclerosing adenosis. When examining a small portion of a focus of sclerosing adenosis, one may not be able to appreciate the lobular organization of the process. In this circumstance, one could mistake a focus of sclerosing adenosis for an invasive lobular carcinoma. Differential Diagnosis: Invasive carcinoma (more atypical, infiltrative, less circumscribed) Discussion: Sclerosing adenosis originates in the center of normally formed lobules, where the glandular proliferation and matrix deposition surround the intralobular terminal ductule. |
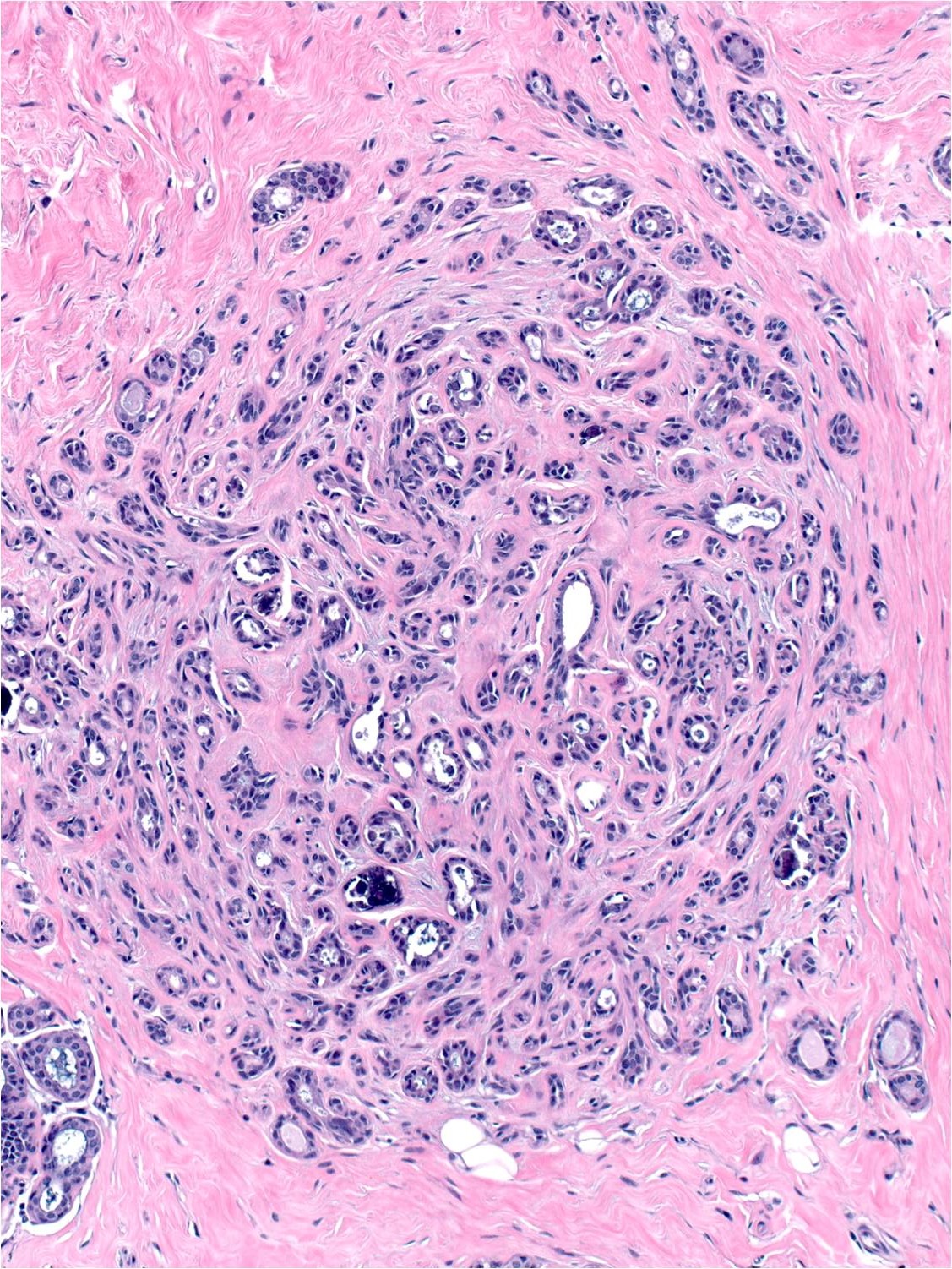 |
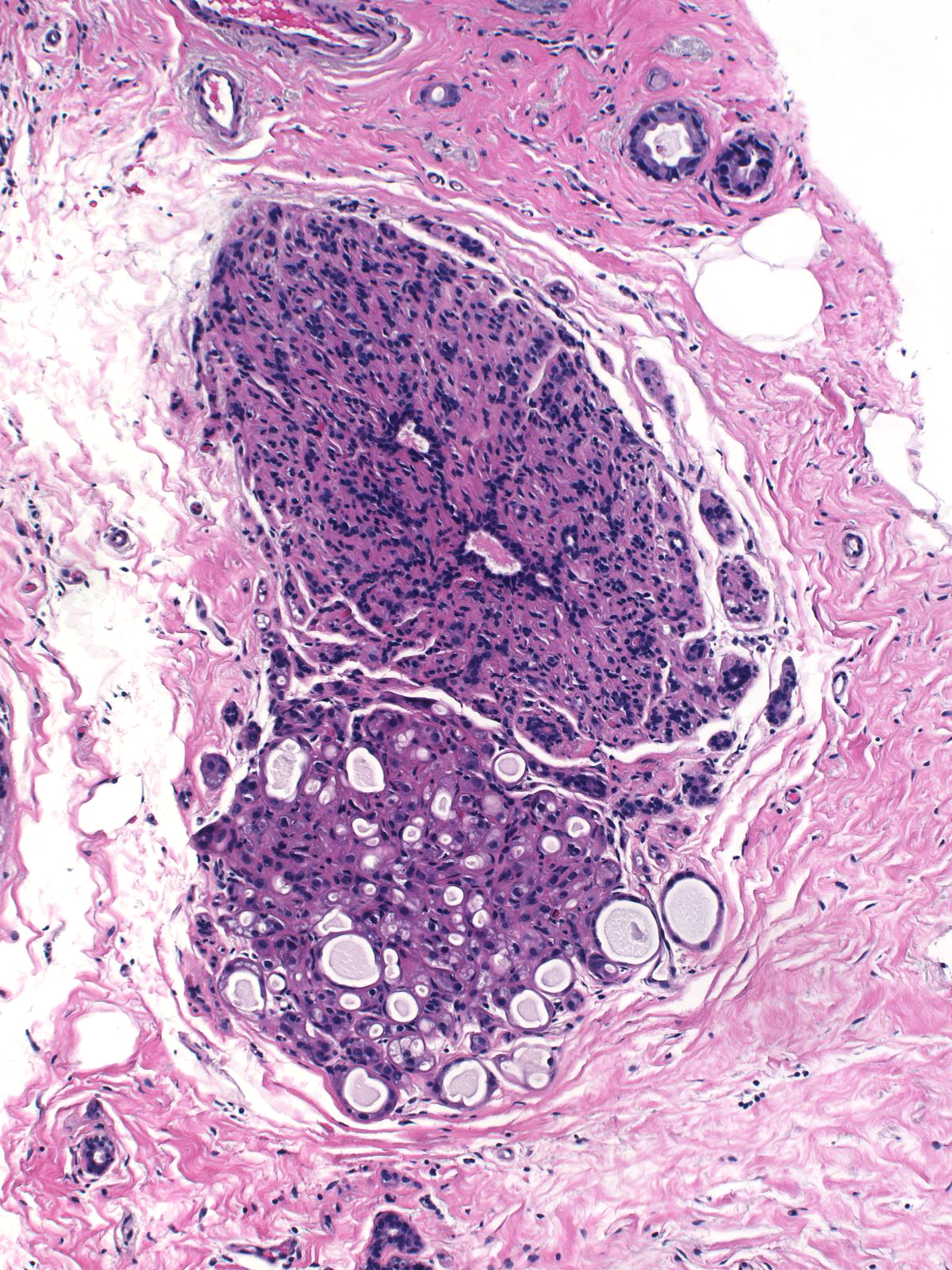
| Flattened glands and eosinophilic extracellular matrix surround the intralobular terminal ductule in this affected lobule. | 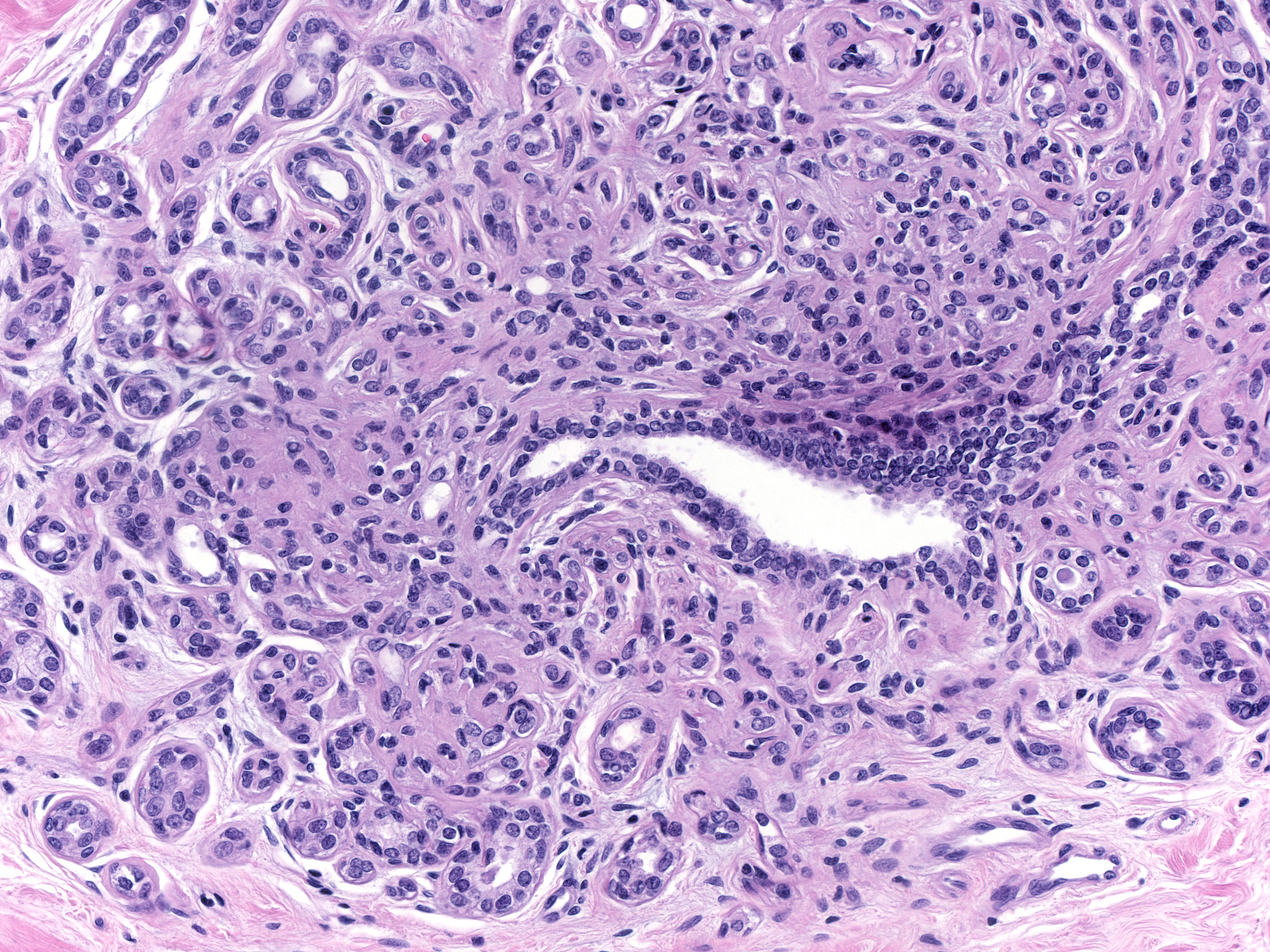 |
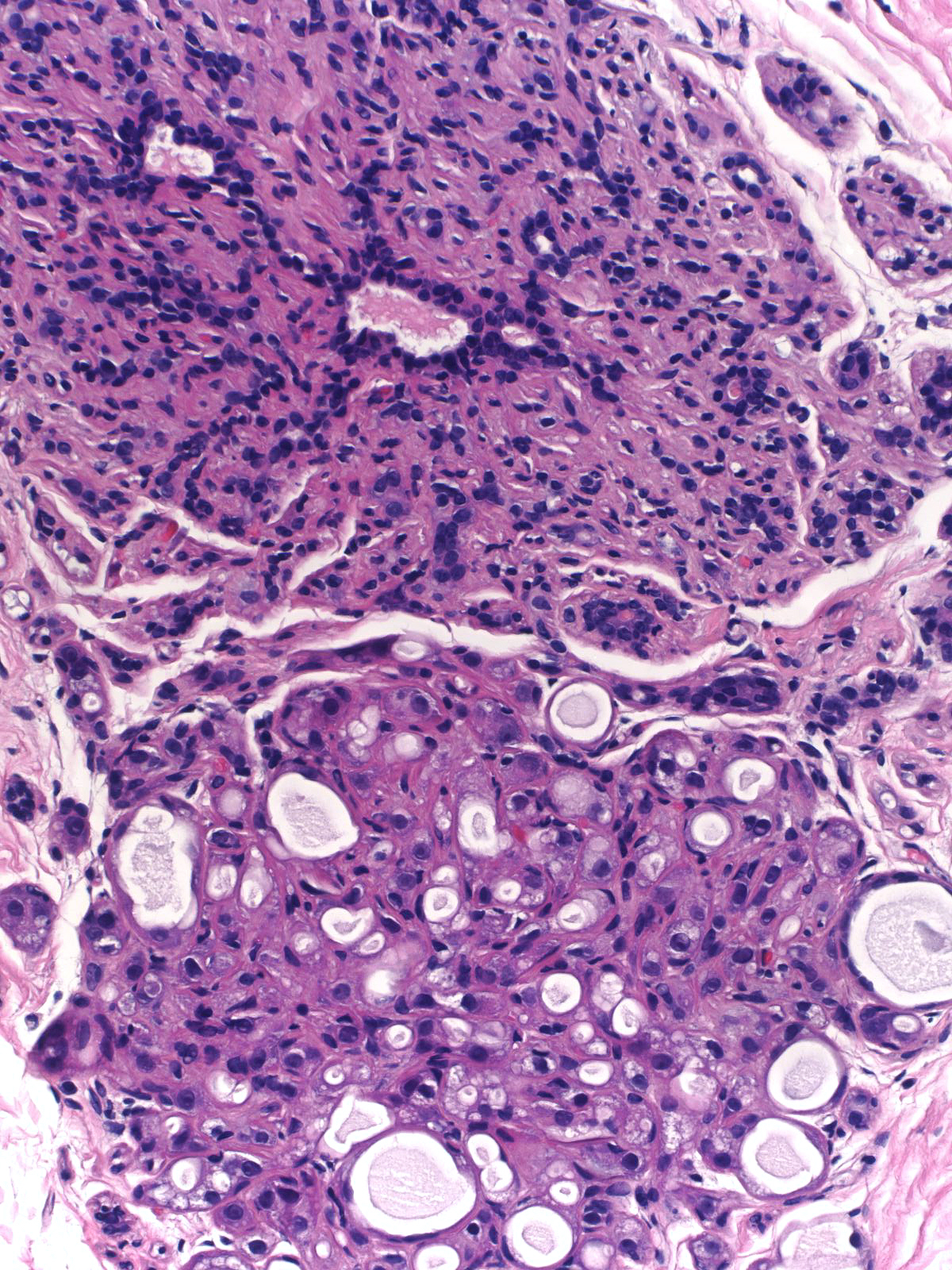
| Near the center of the lesion, compression of the tubules makes it virtually impossible to identify the lumens of the tubules in most cases. | 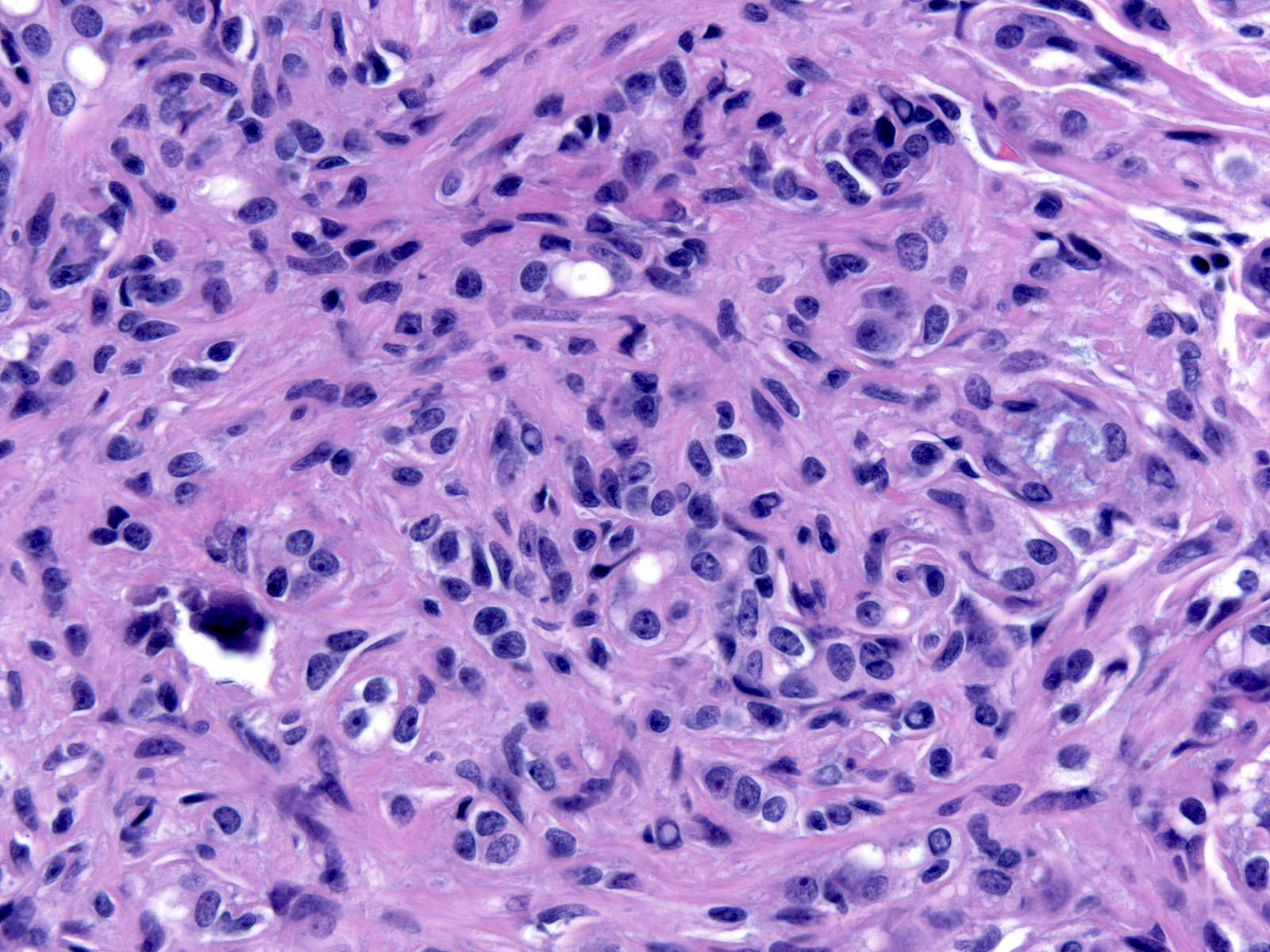 |
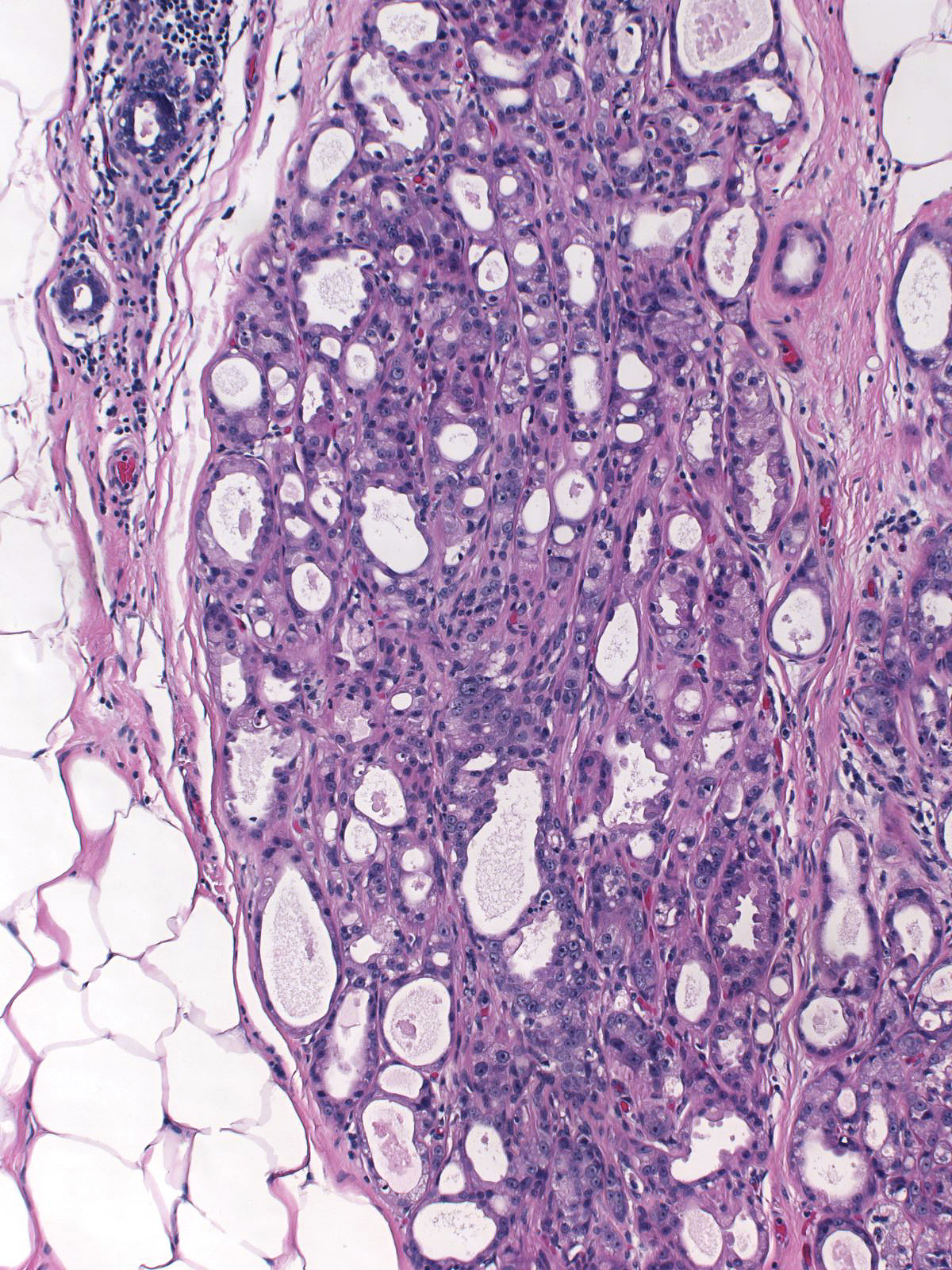
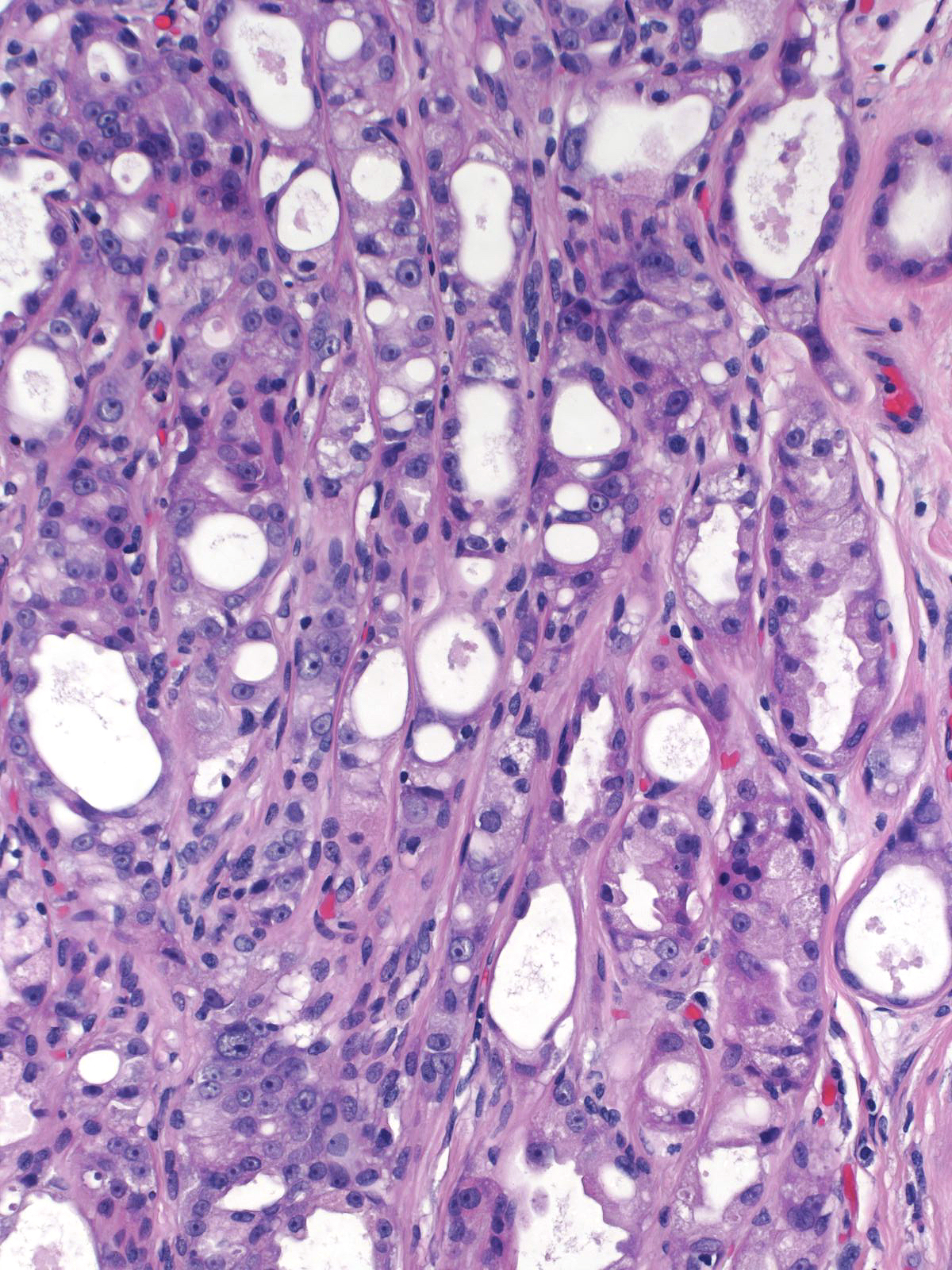
| Although highly compressed, careful inspection and immunohistochemical staining of the tubules will reveal the presence of both luminal and myoepithelial cells distributed in their proper arrangement. In certain areas, often at the edge of the lesion, it is easier to appreciate the slender tubules. | 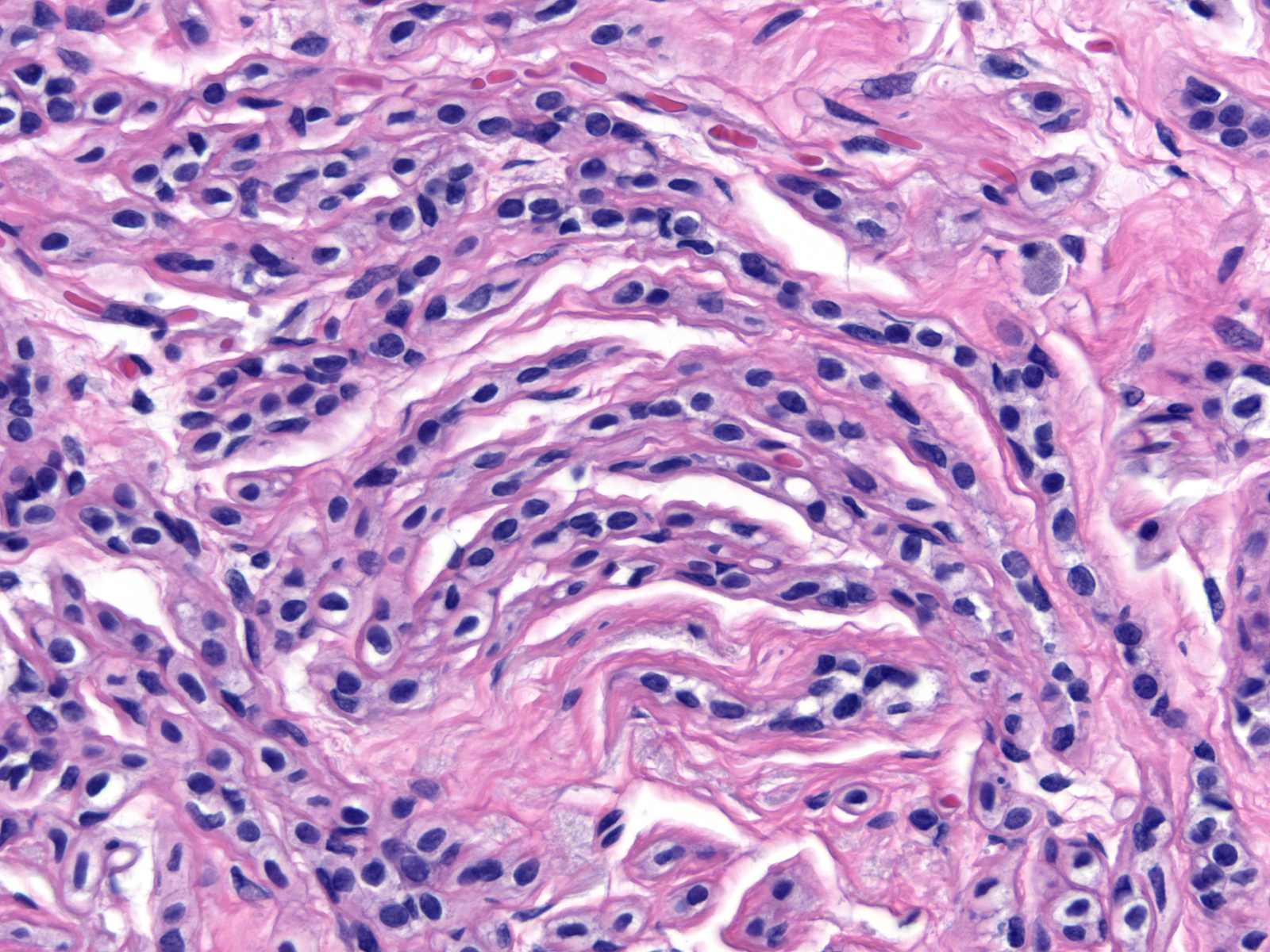 |
| The process does not usually involve the entire lobule; consequently, a few unaltered acini may remain along its perimeter. | 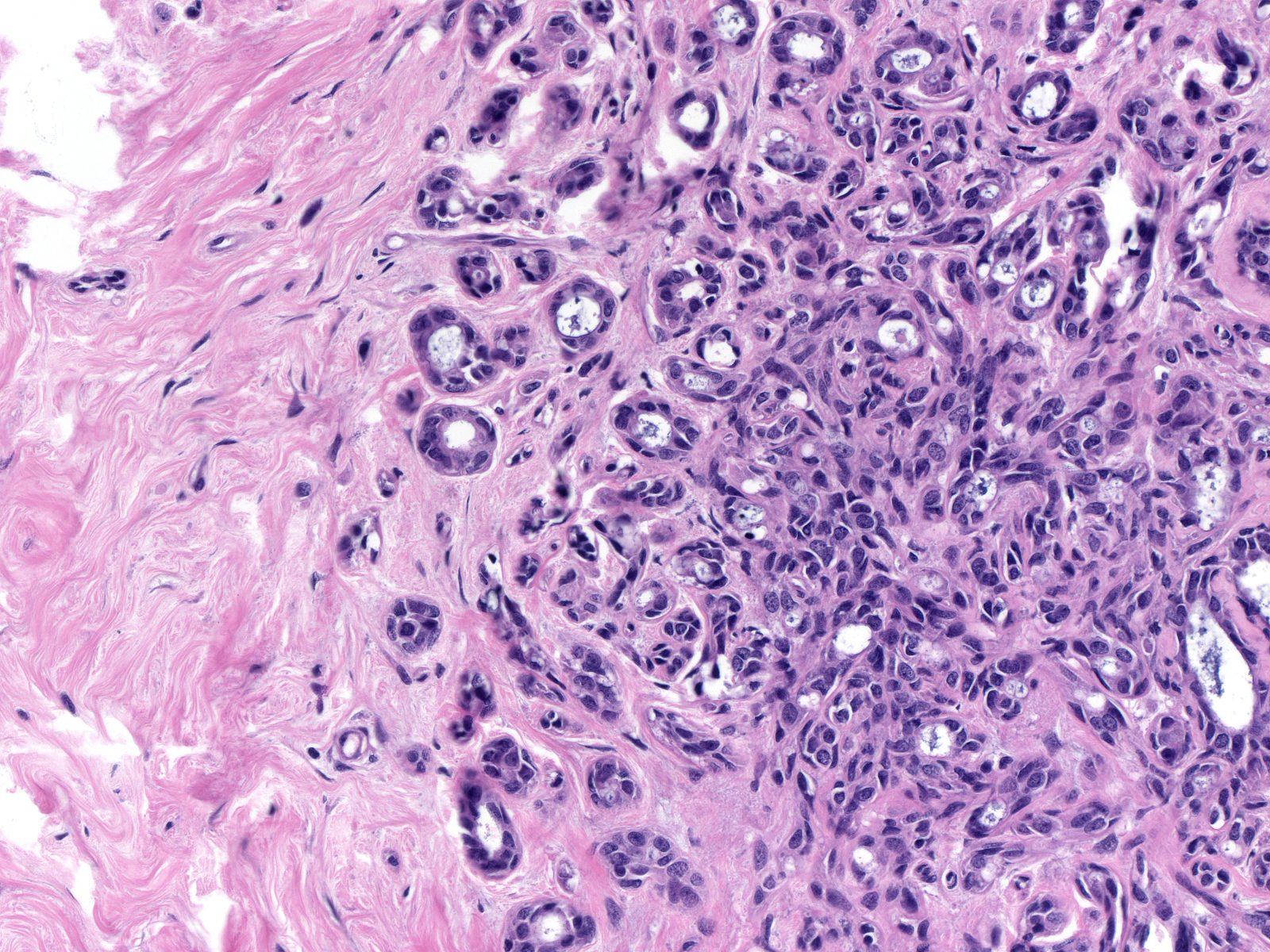 |
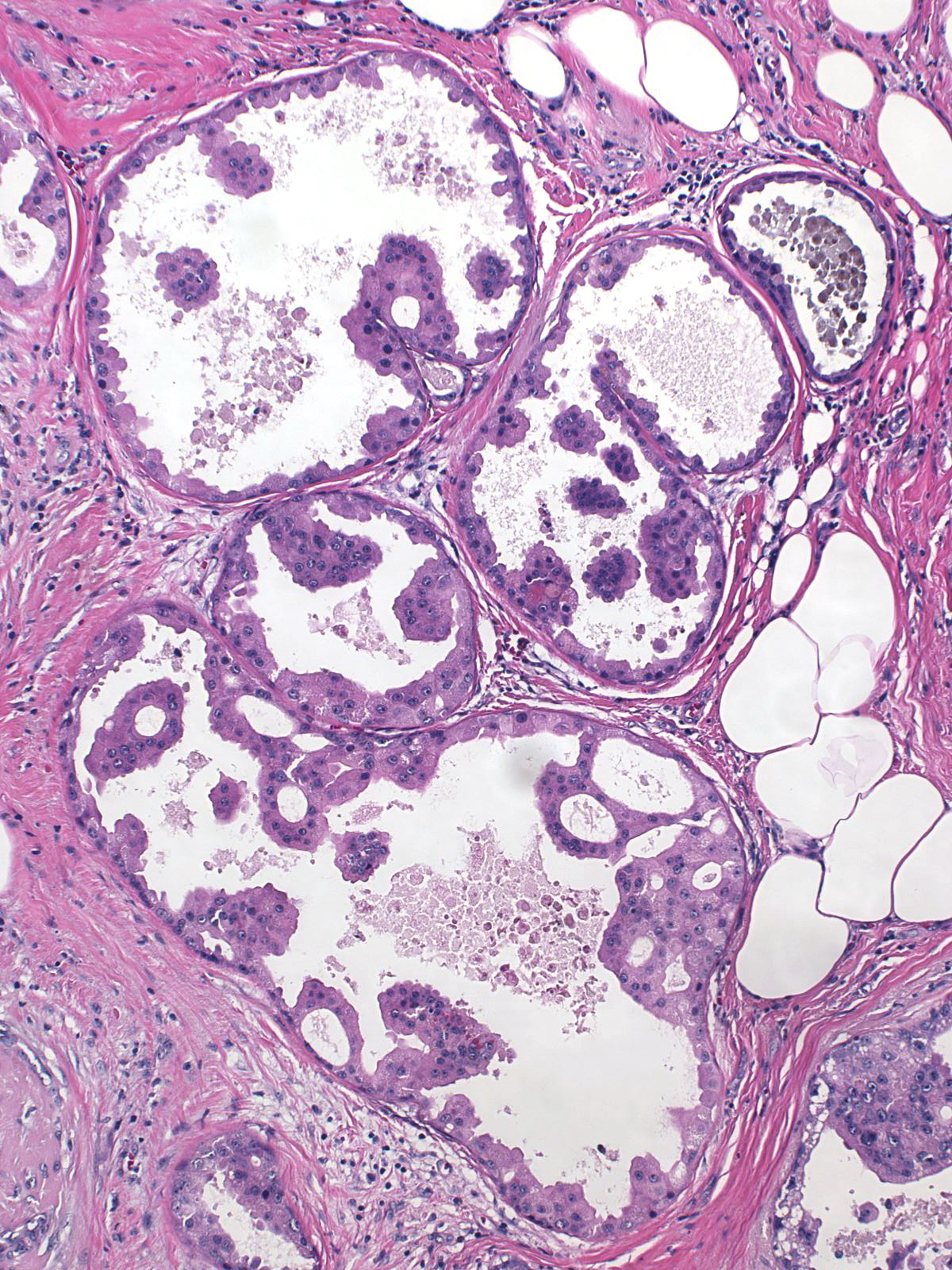
| Often, sclerosing adenosis involves multiple lobules arising along the course of a small duct. | 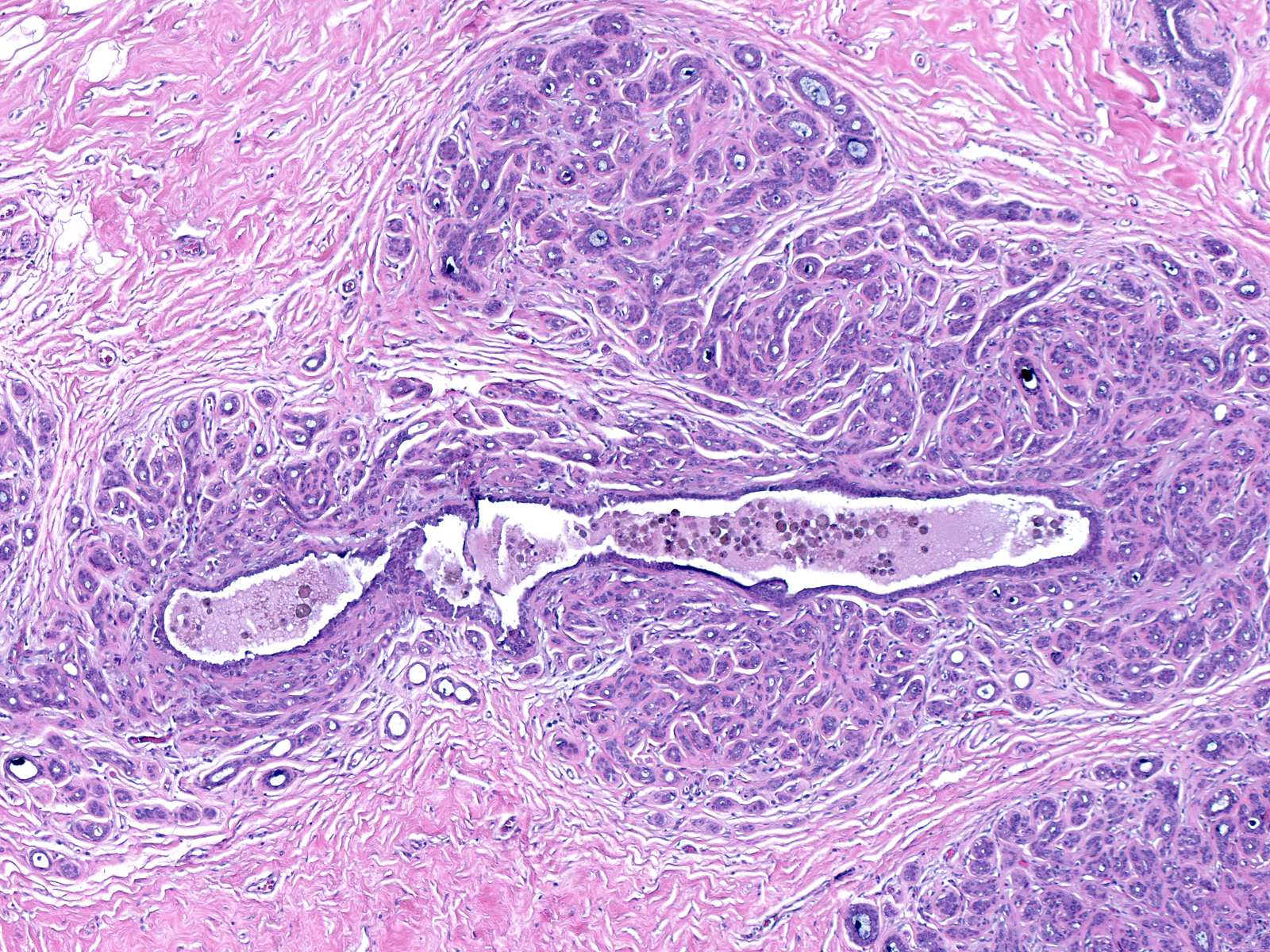 |
| Here, three lobules affected by the process have begun to merge together. Confluence of the process in adjacent lobules can lead to the formation of larger areas of sclerosing adenosis and, eventually, the presence of a palpable mass. | 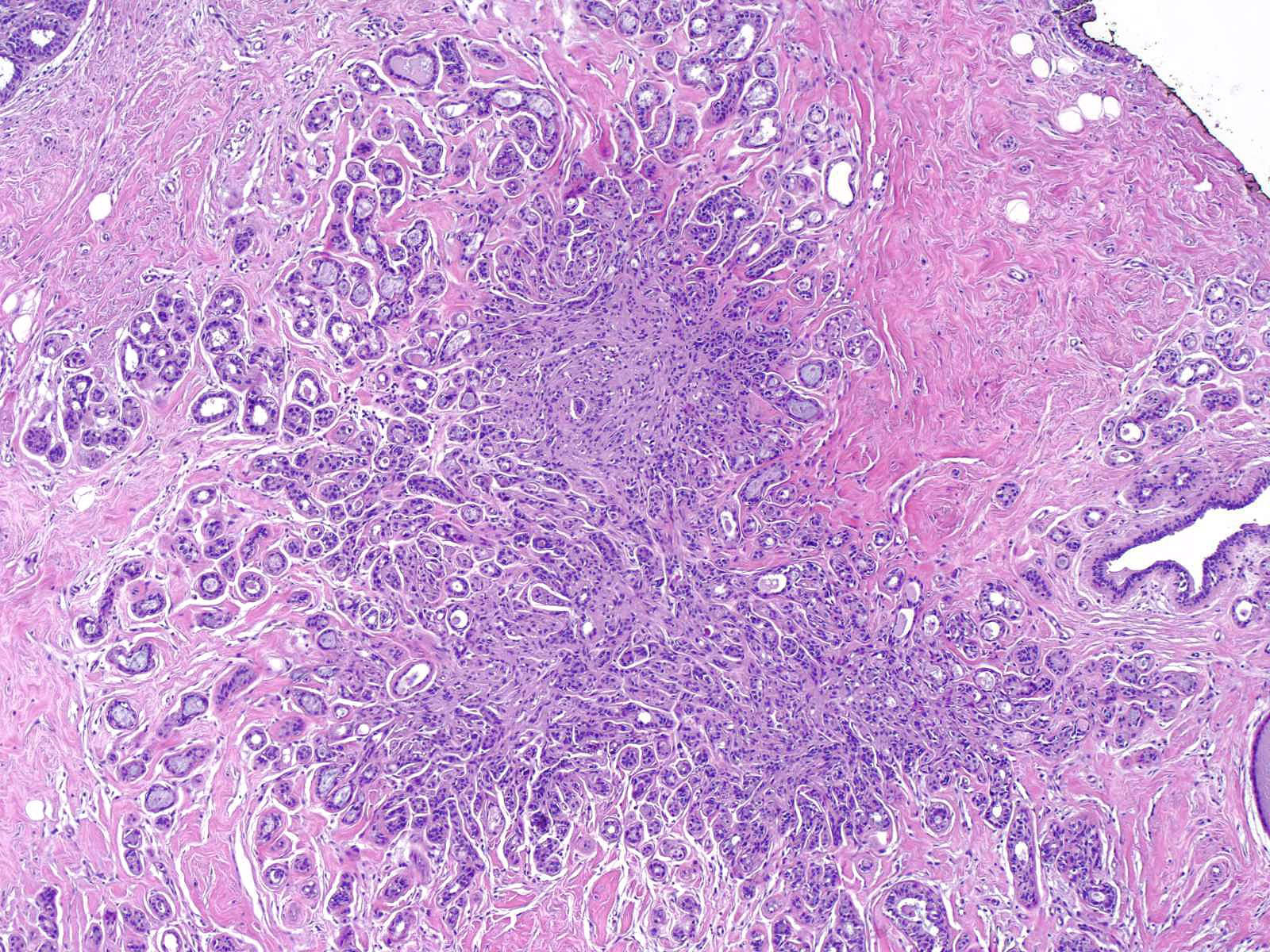 |
| Atrophy in regions of sclerosing adenosis can give rise to an appearance that resembles invasive carcinoma. Glandular atrophy causes the disappearance of the peripheral preserved acini, and atrophy of the nonspecialized stroma leads to its replacement by fat. Because of these changes, the compressed cords of cells seem to extend between the adipocytes. | 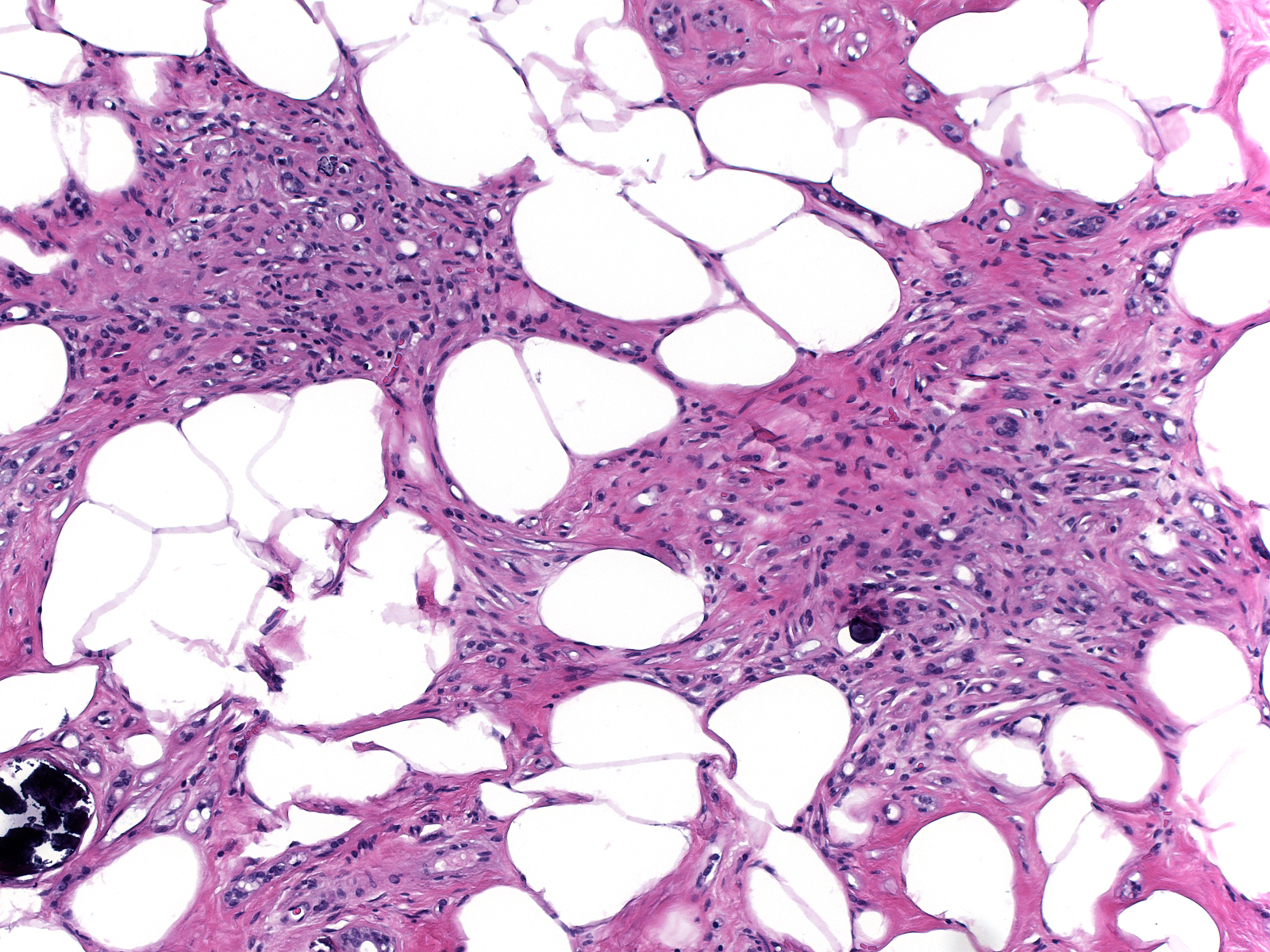 |
When atypical apocrine cells take up residence in foci of sclerosing adenosis, pathologists refer to the lesion as atypical apocrine adenosis.
In this example, the atypical cells occupy a portion of this focus of sclerosing adenosis (left). The atypical apocrine cells appear larger than the normal cells and the possess abundant eosinophilic cytoplasm and nuclei of varying size and shape, which contain prominent nucleoli and display thick membranes (right). The nuclear pleomorphism and cytoplasmic vacuolization represent manifestations of cytological atypia.
 |
 |
Foci of atypical apocrine adenosis often co-exist with more common forms of epithelial atypia such as lobular neoplasia and atypical ductal hyperplasia. This focus of atypical apocrine adenosis (left and center) sat next to a focus of apocrine ductal carcinoma in-situ (right).
 |
 |
 |