Difference between revisions of "Medullary Carcinoma"
(Created page with "__NOCACHE__{{DISPLAYTITLE:Medullary Carcinoma}} {{:TOC}} == General == Image:26-1 Med.jpg|thumb|The diagnosis of medullary carcinoma requires strict adherence to its histolo...") |
|||
| (One intermediate revision by one other user not shown) | |||
| Line 1: | Line 1: | ||
| − | __NOCACHE__ | + | __NOCACHE__ |
{{:TOC}} | {{:TOC}} | ||
| − | == | + | <br> |
| − | + | == Introduction == | |
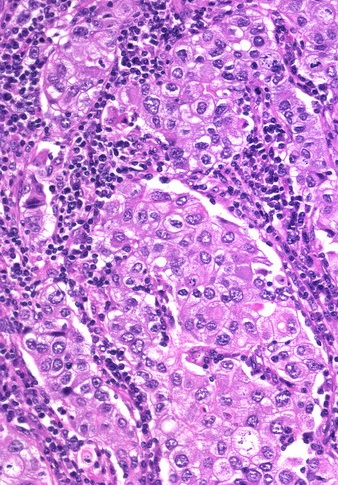
| − | + | {{dxintro|Medullary Carcinoma|Medullary carcinoma is a type of invasive ductal carcinoma characterized by circumscription, high-grade atypia, and marked chronic inflammation.|Medullary carcinoma usually presents as a mass and it tends to afflict women younger than fifty years. Almost never does it arise in men. Spread to axillary lymph nodes occurs less commonly than it does with conventional carcinomas. Patients with medullary carcinoma have a more favorable prognosis than those with high-grade invasive ductal carcinomas of comparable grade and stage.|Medullary carcinomas form a moderately firm, well defined lobulated mass, which can mimic a benign nodule.|The carcinoma grows as a circumscribed mass, often subdivided into nodules by fibrous bands. Chronic inflammatory cells surround the mass and penetrate into its interior. The carcinoma cells form a syncytial mass and they display anaplastic cytological features and frequent mitotic figures. The carcinoma cells typically do not stain for estrogen receptors. The presence of these receptors should lead one to reconsider the diagnosis of medullary carcinoma.|High-grade invasive ductal carcinoma (does not meet diagnostic criteria)|Studies conducted in the past several decades revealed marked interobserver variability regarding the diagnosis of medullary carcinoma. Because of this poor reproducibility, pathologists at MGH have abandoned this diagnosis except in rare instances. One must restrict the diagnosis of medullary carcinoma to cases showing all the following histological features: | |
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
** 1. Syncytial growth in at least 75% of the mass (The tumor cells must form broad sheets or nests composed of cells with indistinct borders. The indistinct quality of the cell borders makes the cells look multinucleate. (A syncytium is a multinucleate cell formed by the fusion of uninucleate cells.)) | ** 1. Syncytial growth in at least 75% of the mass (The tumor cells must form broad sheets or nests composed of cells with indistinct borders. The indistinct quality of the cell borders makes the cells look multinucleate. (A syncytium is a multinucleate cell formed by the fusion of uninucleate cells.)) | ||
** 2. Noninvasive microscopic circumscription (The edge of the tumor must have a smooth, rounded contour that appears to push aside the breast parenchyma and fat rather than to invade it.) | ** 2. Noninvasive microscopic circumscription (The edge of the tumor must have a smooth, rounded contour that appears to push aside the breast parenchyma and fat rather than to invade it.) | ||
** 3. Anaplastic cytological features (The carcinoma cells must appear large and they must possess large pleomorphic nuclei and large nucleoli.) | ** 3. Anaplastic cytological features (The carcinoma cells must appear large and they must possess large pleomorphic nuclei and large nucleoli.) | ||
** 4. Prominent chronic inflammatory cell infiltrate around and within the mass | ** 4. Prominent chronic inflammatory cell infiltrate around and within the mass | ||
| − | ** 5. High mitotic rate | + | ** 5. High mitotic rate|26-1 Med.jpg|The diagnosis of medullary carcinoma requires strict adherence to its histologic criteria.}} |
| + | |||
<br> | <br> | ||
Ductal carcinoma in-situ often occupies ducts and lobules surrounding the mass. Independent foci of invasion originating from the involved ducts can give rise to satellite nodules of invasive carcinoma. | Ductal carcinoma in-situ often occupies ducts and lobules surrounding the mass. Independent foci of invasion originating from the involved ducts can give rise to satellite nodules of invasive carcinoma. | ||
<br> | <br> | ||
In the past, pathologists have classified carcinomas showing many of, but not all, the features of medullary carcinoma as atypical medullary carcinomas or carcinomas with medullary features. The authors of the current WHO classification eliminated the categories of medullary carcinoma and atypical medullary carcinoma and classify all high‑grade invasive ductal carcinomas with a prominent chronic inflammatory cell infiltrate as carcinoma with medullary features. | In the past, pathologists have classified carcinomas showing many of, but not all, the features of medullary carcinoma as atypical medullary carcinomas or carcinomas with medullary features. The authors of the current WHO classification eliminated the categories of medullary carcinoma and atypical medullary carcinoma and classify all high‑grade invasive ductal carcinomas with a prominent chronic inflammatory cell infiltrate as carcinoma with medullary features. | ||
| − | + | {{:mgh:breast-footer}} | |
| − | |||
| − | |||
Latest revision as of 09:32, July 17, 2020
Contents
Introduction
|
Definition: Medullary carcinoma is a type of invasive ductal carcinoma characterized by circumscription, high-grade atypia, and marked chronic inflammation. Clinical Significance: Medullary carcinoma usually presents as a mass and it tends to afflict women younger than fifty years. Almost never does it arise in men. Spread to axillary lymph nodes occurs less commonly than it does with conventional carcinomas. Patients with medullary carcinoma have a more favorable prognosis than those with high-grade invasive ductal carcinomas of comparable grade and stage. Gross Findings: Medullary carcinomas form a moderately firm, well defined lobulated mass, which can mimic a benign nodule. Microscopic Findings: The carcinoma grows as a circumscribed mass, often subdivided into nodules by fibrous bands. Chronic inflammatory cells surround the mass and penetrate into its interior. The carcinoma cells form a syncytial mass and they display anaplastic cytological features and frequent mitotic figures. The carcinoma cells typically do not stain for estrogen receptors. The presence of these receptors should lead one to reconsider the diagnosis of medullary carcinoma. Differential Diagnosis: High-grade invasive ductal carcinoma (does not meet diagnostic criteria) Discussion: Studies conducted in the past several decades revealed marked interobserver variability regarding the diagnosis of medullary carcinoma. Because of this poor reproducibility, pathologists at MGH have abandoned this diagnosis except in rare instances. One must restrict the diagnosis of medullary carcinoma to cases showing all the following histological features:
|
 |
Ductal carcinoma in-situ often occupies ducts and lobules surrounding the mass. Independent foci of invasion originating from the involved ducts can give rise to satellite nodules of invasive carcinoma.
In the past, pathologists have classified carcinomas showing many of, but not all, the features of medullary carcinoma as atypical medullary carcinomas or carcinomas with medullary features. The authors of the current WHO classification eliminated the categories of medullary carcinoma and atypical medullary carcinoma and classify all high‑grade invasive ductal carcinomas with a prominent chronic inflammatory cell infiltrate as carcinoma with medullary features.